Received: Mon 07, Jul 2025
Accepted: Mon 21, Jul 2025
Abstract
Previous studies have described disparities among Spanish-speaking patients (SSPs) compared to their English-speaking counterparts across various fields of medicine. However, there exists a paucity of evidence regarding these disparities within neurosurgery. Moreover, there is a need to identify specific discrepancies between SSPs and English-speaking patients (ESPs) to enact specific interventions to improve these outcomes. To accomplish this goal, the present study was conducted to compare differences in hospital course and postoperative complications between SSPs and ESPs following shunt placement for hydrocephalus. This two-center retrospective cohort study included adult patients (≥18 years) who underwent initial shunt placement for hydrocephalus (excluding normal pressure hydrocephalus) between January 1, 2016, and December 31, 2023, and who primarily spoke English or Spanish. Primary outcomes were postoperative complications and 30-day readmission. Secondary outcomes included length of stay (LOS), extraventricular drain (EVD) placement, intensive care unit (ICU) admission, and pain management at discharge. Among 206 patients (mean age 50.9 ± 2.3 years; 48.1% female), 32 were SSPs and 174 were ESPs. SSPs had higher rates of prior stroke (p = 0.003), lower median household income (p = 0.0008), and were more likely to be never-smokers (p = 0.011). After adjusting for confounders using Poisson and linear regression, SSPs had higher rates of EVD placement (RR 1.56, 95% CI 1.17-2.09; p = 0.003), ICU admission (RR 1.90, 95% CI 1.25-2.90; p = 0.003), and longer LOS (β = 10.53 days, 95% CI 1.32-19.75; p = 0.025). SSPs were also less likely to be discharged with pain medications (p = 0.014). Despite these differences, SSPs had significantly lower 30-day readmission rates than ESPs (RR 0.27, 95% CI 0.07-0.98; p = 0.046), with no significant difference in complication rates. In a 1:3 propensity-matched analysis (16 SSPs, 48 ESPs), SSPs remained more likely to undergo EVD placement (p = 0.041) and had an increased 9-hour median difference from admission to EVD placement compared to ESPs (p = 0.037). Though generalizability may be limited by the small sample size, these results identify several areas where specific interventions such as increased culturally tailored patient education materials, clinician cultural humility training, and increased access to quality interpretation services could improve existing disparities between SSPs and ESPs within neurosurgery.
Keywords
Ventriculoperitoneal shunts, hydrocephalus, language
1. Introduction
Hydrocephalus is a complex neurological condition characterized by an increase in cerebrospinal fluid (CSF) volume, leading to ventricular dilation and potentially increased intracranial pressure (ICP) [1]. In adults, complications of hydrocephalus and its treatment can be severe, including brain herniation and death [2]. Neurosurgical intervention, typically via ventriculoperitoneal shunt placement, is often required [2-5]. While clinical factors affecting outcomes in hydrocephalus have been well described, limited research has addressed how social determinants of health, particularly language, may influence perioperative care and outcomes in adult patients undergoing surgery for hydrocephalus. Though some work has explored this issue in pediatric populations, evidence regarding the impact of primary language on adult neurosurgical outcomes remains limited [6-11].
This gap is especially relevant given the changing demographics of the U.S. In 2020, the Hispanic population reached 62.1 million, comprising 19% of the total population and representing the nation’s second-largest ethnic group [12]. Additionally, the Hispanic population is among the fastest-growing groups in the U.S., increasing by 23% from 50.5 million in 2010 to 62.1 million in 2020 [13]. Within this population, nearly 17 million individuals, approximately one in four Spanish speakers, have limited English proficiency (LEP) [14]. Prior studies have identified multiple barriers that Spanish-speaking patients (SSPs) face in accessing and navigating healthcare systems, including poor understanding of diagnoses, mistrust of providers, and lower satisfaction with care [15]. These challenges have been linked to tangible disparities such as difficulty securing appointments, inadequate postoperative pain control, longer hospital stays, and increased complication rates across various medical specialties [16-18].
Despite robust evidence of worse outcomes for SSPs in other fields, a paucity of data exists within the neurosurgical literature regarding this population, particularly in the adult population with hydrocephalus. Of the pertinent studies that do exist, evidence suggests that the current management of SSPs with hydrocephalus is suboptimal. A recent study found that pediatric SSPs undergoing neurosurgical management for hydrocephalus had poorer postoperative follow-up than English-speaking patients (ESPs), placing them at a higher risk for complications [8]. However, little is known about how language barriers may shape the perioperative course itself, including the use of intensive care, procedural delays, and discharge planning. Understanding these patterns is critical for identifying specific, actionable targets to improve care delivery and advance health equity in neurosurgery.
This study aims to evaluate and compare clinical outcomes between adult SSPs and ESPs undergoing shunt placement for hydrocephalus. We investigated rates of external ventricular drain (EVD) placement, intensive care unit (ICU) admission, total hospital length of stay (LOS), ICU LOS, pain management at discharge, postoperative complications, 30-day readmission, and discharge disposition. In addition to characterizing disparities in management, we aim to inform future interventions that may promote more equitable care for linguistically diverse neurosurgical patients.
2. Materials and Methods
2.1. Study Design
This was a two-center retrospective cohort study conducted in large, tertiary care trauma centers. We reviewed patient charts to analyze outcomes of adults (≥18 years) treated with a shunt for hydrocephalus. This study was conducted with approval from the Banner Health Institutional Review Board. Patients were first identified by International Classification of Diseases-Tenth Revision (ICD-10) codes G91.0, G91.1, and G91.3-G91.9. Patients were included if diagnosed with any hydrocephalus except normal pressure hydrocephalus (NPH) and underwent initial shunt placement at Banner University Medical Center-Phoenix and Banner University Medical Center-Tucson between January 1, 2016, and December 31, 2023. Given that NPH is a more chronic condition and has a different pathophysiology than other forms of hydrocephalus, these patients were excluded to minimize underlying confounding variables. In cases where the nonspecific code G91.9 (unspecified hydrocephalus) was listed alongside a more specific diagnosis, only the specific code was used for classification. Patients’ primary language was determined by the preferred language listed in their chart and only English or Spanish speakers were included. Any patient who did not receive a shunt was excluded. Primary outcomes included postoperative complications and readmission to the Banner Hospital system within 30 days of discharge. Secondary outcomes included EVD placement, ICU admission, LOS, ICU LOS, pain management at discharge, and discharge disposition.
2.2. Data Collection
After patients were identified, patient data were collected, de-identified, and stored using REDCap (Research Electronic Data Capture), hosted at the University of Arizona [19, 20]. Chart reviews were conducted using PowerChart to gather information across several categories: demographics; preoperative history; operative information; and postoperative course. ZIP codes were recorded for each available patient to determine median household income. The United States Census Bureau website was referenced to determine the median household income by ZIP code using the 2022 American Community Service Survey [21]. Interpreter status was determined based on physician documentation. Patients whose records indicated the presence of a professional interpreter were categorized as having a certified medical interpreter. Those documented as using a family member or untrained individual were classified as having an ad hoc interpreter. A language-concordant surgeon was defined as a provider fluent in Spanish, as identified through institutional bios or public consumer health websites. If no interpreter status was noted and the surgeon did not speak Spanish, the encounter was categorized as undocumented. Insurance status was determined by the primary listed insurance provider: private payer, Medicaid/Arizona Health Care Cost Containment System (AHCCCS), Medicare, uninsured, and other types of insurance. Intraoperative complications were determined by documented complications within the operative note and post-operative chart review. Pain management at discharge was determined by documented medications in the patient’s discharge paperwork.
2.3. Statistical Analysis
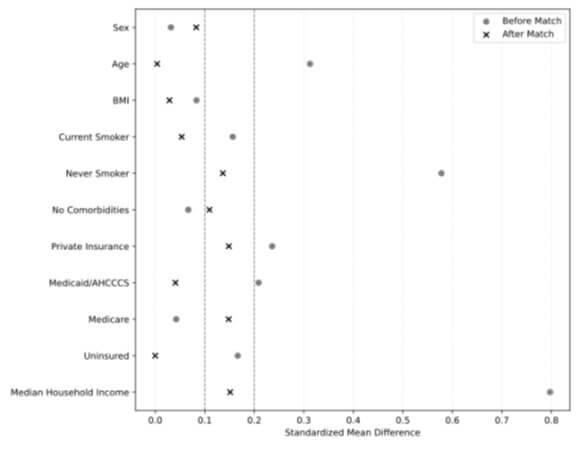
All analyses and figures were generated using Python 3.12.3 using relevant packages (e.g., statsmodels, scipy, etc.). Demographic data including age, body mass index (BMI), and median household income were compared using the Mann-Whitney U due to non-normal distribution. Sex, insurance status, comorbidities, smoking status, and type of hydrocephalus were compared using a chi-squared test of independence. EVD placement, ICU admission, pain management at discharge, 30-day readmission, discharge disposition, and postoperative complications were compared using the chi-square test of independence, Fisher’s exact test, and a Poisson regression with robust standard errors to estimate relative risk (RR) and 95% confidence intervals (CI). Given the larger number of possible postoperative complications, a Benjamini-Hochberg False Discovery Rate (FDR) was calculated to decrease the likelihood of Type I error. FDR values less than 0.05 were considered statistically significant. Time from admission to EVD placement, EVD placement to shunt placement, LOS, and ICU LOS were compared using a Mann-Whitney U test and multiple linear regression. Patients were excluded from regression analyses if they lacked one or more included variables for a given outcome of interest. Additionally, a propensity match was conducted to reduce confounding due to baseline differences between SSPs and ESPs. A propensity score (PS) was estimated using logistic regression. The PS model included covariates such as age, sex, BMI, smoking status, presence of comorbidities, type of insurance, and median household income. The dependent variable was language group (SSP vs. ESP), and the model predicted the probability of a patient being in the SSP group given their observed characteristics. These propensity scores were then used to perform a 1:3 nearest-neighbor matching with a caliper of 0.05 to balance covariates across groups and create a matched sample for outcome comparison. Standardized mean differences (SMD) were calculated before and after matching to ensure proper standardization of each covariate and were plotted on a Love plot for visualization. EVD placement, ICU admission, complication rate, any pain medication at discharge, 30-day readmission to the same hospital system, and discharge disposition were all analyzed using Fisher’s exact test given the reduced sample size following propensity matching. Time from admission to EVD, EVD placement to shunt placement, LOS, and ICU LOS were analyzed using Mann-Whitney U.
3. Results
3.1. Demographics
A total of 206 patients (32 SSPs and 174 ESPs) were included in the study, with a mean age of 50.90 ± 2.32 years and 99 (48.1%) identified as female. The median age was 55.50 years for SSPs and 52.00 years for ESPs. Females comprised 50.00% of the SSP group and 52.30% of the ESP group. Among patients with available BMI data, the median BMI was 26.29 for SSPs and 27.10 for ESPs; BMI data were missing for 6 SSPs and 41 ESPs (Table 1). There was no significant difference in insurance status or the overall burden of comorbidities between groups, except for a higher prevalence of prior cerebrovascular accidents in the SSP group (p = 0.003). There were no statistically significant differences between groups in the distribution of hydrocephalus subtypes (p > 0.1). Smoking status differed significantly between groups (p = 0.011), with SSPs more likely to report never smoking (88.90% vs. 63.40%). Lastly, SSPs had significantly lower estimated median household incomes compared to ESPs (p = 0.0008); income data was unavailable for the ZIP codes of one SSP and four ESPs. Interpreter use among SSPs was variably documented in the medical record. Of the 32 SSPs, 34.38% were noted to have had encounters with certified medical interpreters, 15.63% used ad hoc interpreters, 15.63% were treated by a language-concordant surgeon, and for 34.38%, interpreter status was undocumented.
Table.
1. Baseline
demographic characteristics of Spanish-speaking and English-speaking patients
who underwent shunt placement for treatment of hydrocephalus.
|
Spanish
(n=32) |
English
(n=174) |
p-value |
|
|
Female
(%) |
50.00 |
52.30 |
0.963 |
|
Age
(years, median, IQR) |
55.50 (45.75-69.00) |
52.00
(36.25-64) |
0.215 |
|
BMI
(kg/m2, median, IQR) † |
26.29
(23.518-30.338) |
27.10
(22.86-30.9) |
0.950 |
|
Median
Household Income by ZIP Code ($, median, IQR) †† |
55771
(47208-68376) |
69087
(55461-93435) |
0.0008** |
|
Insurance
Status |
0.603 |
||
|
Private
Insurance |
22.60 |
33.33 |
- |
|
Medicaid/AHCCCS |
48.40 |
42.00 |
- |
|
Medicare |
19.40 |
19.00 |
- |
|
Uninsured/Other |
9.70 |
5.70 |
- |
|
Comorbidities
(%) |
|||
|
DM |
15.60 |
13.80 |
1.000 |
|
HTN |
56.20 |
40.20 |
0.136 |
|
Dyslipidemia/Hypercholesterolemia |
28.10 |
13.20 |
0.061 |
|
COPD |
3.10 |
2.30 |
1.000 |
|
Epilepsy/Seizures |
9.40 |
6.90 |
0.900 |
|
Current
CA |
12.50 |
11.50 |
1.000 |
|
Previous
CA |
3.10 |
8.00 |
0.539 |
|
Dementia |
0.00 |
1.10 |
1.000 |
|
Heart
Disease/Arrythmias |
15.60 |
8.00 |
0.303 |
|
CVA |
18.80 |
3.40 |
0.003** |
|
Hypothyroidism |
6.20 |
6.30 |
1.000 |
|
CKD/Renal
Failure |
3.10 |
4.00 |
1.000 |
|
Meningitis |
6.20 |
9.80 |
0.764 |
|
Previous
Brain Hemorrhage |
9.40 |
5.20 |
0.602 |
|
TBI |
3.10 |
5.20 |
0.962 |
|
Coccidioidomycosis |
6.20 |
9.80 |
0.764 |
|
HIV |
0.00 |
5.20 |
0.398 |
|
Other |
37.50 |
41.40 |
0.830 |
|
None |
12.50 |
14.40 |
0.998 |
|
Hydrocephalus
Type (%), ICD-10 |
|
|
|
|
Communicating
(G91.0) |
9.40 |
23.00 |
0.132 |
|
Obstructive
(G91.1) |
28.10 |
20.10 |
0.435 |
|
Post-traumatic
(G91.3) |
6.20 |
4.60 |
1.000 |
|
Hydrocephalus
in disease classified elsewhere (G91.4) |
3.10 |
1.10 |
0.957 |
|
Hydrocephalus,
unspecified (G91.9) |
53.10 |
51.70 |
1.000 |
|
Smoking
Status (%)††† |
|
|
0.011* |
|
Current
Smoker |
10.00 |
20.20 |
- |
|
Non-Smoker |
10.00 |
29.20 |
- |
|
Never
Smoker |
88.90 |
63.40 |
- |
IQR: Interquartile Range, AHCCCS: Arizona Health Care Cost Containment System, DM: Diabetes Mellitus, HTN: Hypertension, COPD: Chronic Pulmonary Obstructive Disease, CA: Cancer, CVA: Cerebrovascular Accident; CKD: Chronic Kidney Disease; TBI: Traumatic Brain Injury; HIV: Human Immunodeficiency Virus; ICD-10: International Classification of Diseases-Tenth Revision, BMI: Body Mass Index. †n=26/133, ††n=31/170, †††n=30/168, *p-value <0.05, **p-value <0.01.
3.2. Univariate Analysis
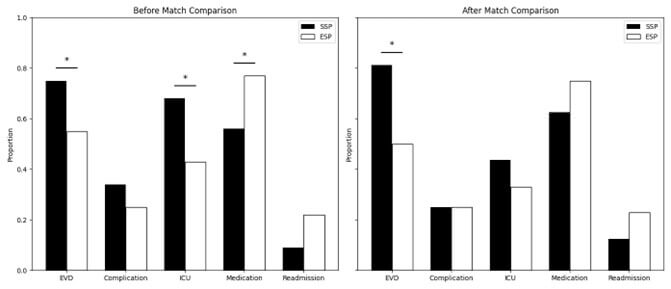
Several significant differences were identified upon initial analysis of the entire sample (Table 2). First, the rate of EVD placement was higher in SSPs (75.00% vs 55.00%) compared to ESPs (p = 0.032). Additionally, the median time to EVD placement was 12.50 hours in SSPs compared to 7.50 hours in ESPs (p = 0.034). However, there was no difference in time from EVD placement to shunt placement. Initially, pressure ulcers were found to be more common in SSPs than ESPs following shunt placement (p = 0.026). However, the FDR was calculated and found to be 0.388, making this finding nonsignificant. ICU admission was higher in SSPs, with 67.74% of patients being admitted versus 43.10% of ESPs (p = 0.011). There was no difference in the median ICU LOS (19.00 vs 18.00 days for SSPs and ESPs, respectively) or the total LOS (20.00 vs 17.50). However, upon discharge from the hospital, SSPs were less likely to receive any form of pain medication compared to ESPs (56.25% vs 77.01%, p = 0.014). Discharge disposition differed between SSPs and ESPs, though none reached the level of statistical significance. SSPs were most likely to be discharged to home (53.13%), followed by acute care or inpatient rehab (IRF) (25.0%), skilled nursing facility (SNF) or nursing home (15.6%), or another setting (6.3%). No SSPs were sent to hospice. Among ESPs, 35.3% were discharged to home, 25.4% to acute care/IRF, 21.4% to SNF, 5.8% to hospice, and 12.1% to other settings. Data about discharge was missing for one ESP. There was no difference in readmission rates to the same hospital system within 30 days between the two groups.
Table.
2. Results of
univariate analysis between Spanish-speaking and English-speaking patients who
underwent a shunt placement for hydrocephalus.
|
Spanish
(n=32) |
English
(n=174) |
p-value |
FDR |
|
|
EVD
Placement (%) |
75.00 |
54.60 |
0.032* |
- |
|
Time
from admission to EVD† (hours, median, IQR) |
12.50
(7.75-32.75) |
7.50
(3.00-23.88) |
0.034* |
- |
|
Time
from EVD to shunt† (hours, median, IQR) |
398.00
(186.00-601.50) |
402.50
(242.50-550.75) |
0.359 |
- |
|
LOS
(days, median, IQR) |
20.00
(4.75-34.75) |
17.50
(5.00-27.00) |
0.159 |
- |
|
ICU
(%) |
67.74 |
43.10 |
0.011* |
- |
|
ICU
LOS†† (days, median, IQR) |
19.00
(5.00-23.00) |
18.00 (5.00-26.00) |
0.409 |
- |
|
Complications
(%) |
|
|
|
|
|
SSSI |
0.00 |
0.57 |
1.000 |
1.000 |
|
DSSI |
0.00 |
1.15 |
1.000 |
1.000 |
|
Seizure |
0.00 |
1.72 |
1.000 |
1.000 |
|
PE |
0.00 |
0.57 |
1.000 |
1.000 |
|
DVT |
0.00 |
0.00 |
1.000 |
1.000 |
|
Pressure
Ulcer |
6.25 |
0.00 |
0.026 |
0.388 |
|
Respiratory
Complication |
6.25 |
2.87 |
0.319 |
1.000 |
|
Kidney
Complication |
0.00 |
1.15 |
1.000 |
1.000 |
|
Shunt
Blockage |
6.25 |
4.02 |
0.642 |
1.000 |
|
Overdrainage |
0.00 |
2.30 |
1.000 |
1.000 |
|
Underdrainage |
0.00 |
4.02 |
0.602 |
1.000 |
|
Hemorrhage |
3.13 |
2.30 |
0.592 |
1.000 |
|
Herniation |
0.00 |
0.00 |
1.000 |
1.000 |
|
Other |
21.88 |
8.05 |
0.054 |
0.407 |
|
None |
65.63 |
74.71 |
0.160 |
0.803 |
|
Pain
Medication at Discharge (%) |
56.25 |
77.01 |
0.014* |
- |
|
Readmission
within 30 Days of Discharge (%) |
9.38 |
21.84 |
0.105 |
- |
|
Discharge
Disposition (%)††† |
|
|
||
|
Home |
53.13 |
35.26 |
0.074 |
- |
|
Acute
care facility/Inpatient Rehabilitation |
25.00 |
5.78 |
1.000 |
- |
|
SNF/Nursing
Home |
15.63 |
25.43 |
0.634 |
- |
|
Hospice |
0.00 |
21.39 |
0.368 |
- |
|
Other |
6.25 |
12.14 |
0.542 |
- |
FDR: Benjamini-Hochberg False Discovery Rate; EVD: Extraventricular Drain; IQR: Interquartile Range; LOS: Length of Stay; ICU: Intensive Care Unit; SSSI: Superficial Surgical Site Infection; DSSI: Deep Surgical Site Infection; PE: Pulmonary Embolism; DVT: Deep Vein Thrombosis; SNF: Skilled Nursing Facility. †n=24/94, ††n=21/74, †††n=32/173, *p-value < 0.05.
3.3. Multivariate Analysis
To further investigate these findings, multivariate Poisson and linear regressions were run for categorical and continuous variables as appropriate (Table 3). Sex, age, BMI, absence of comorbidities, median household income, smoking status, and insurance status were controlled using a Poisson regression to compare SSPs and ESPs while limiting confounding demographic variables. SSPs had significantly increased odds of EVD placement (RR 1.56; 95% CI 1.17-2.09; p = 0.003) and ICU admission (RR 1.90; 95% CI 1.25-2.90; p = 0.003) compared to ESPs. Notably, SSPs demonstrated a significantly lower risk of hospital readmission (RR 0.27; 95% CI 0.07-0.98; p = 0.046). There were no statistically significant differences in postoperative complications (RR 0.92; 95% CI 0.68-1.22; p = 0.557) or pain medication prescription at discharge (RR 0.82; 95% CI 0.60-1.12; p = 0.206) after adjustment. Additionally, while controlling for the same confounding variables, linear regression showed that SSPs had a significantly longer LOS (ß = 10.53; 95% CI 1.32-19.75; p = 0.025). There were no significant differences in the time from admission to EVD placement (p = 0.072), time from EVD to shunt placement (p = 0.530), or ICU length of stay (p = 0.808).
Table.
3. Results of
multivariate regression analysis of Spanish-speaking and English-speaking
patients who underwent a shunt placement for hydrocephalus.
|
Outcome |
Model
Type |
RR/ß
(95% CI) |
p-value |
|
Poisson
Regression Outcomes |
|
|
|
|
EVD
Placement |
Poisson |
1.56 (1.17-2.09) |
0.003** |
|
ICU
Admission |
Poisson |
1.90
(1.25-2.90) |
0.003** |
|
Postoperative
Complications |
Poisson |
0.92
(0.68-1.22) |
0.557 |
|
30-Day
Readmission |
Poisson |
0.27
(0.07-0.98) |
0.046* |
|
Pain
Medication at Discharge |
Poisson |
0.82
(0.60-1.12) |
0.206 |
|
Linear
Regression Outcomes |
|||
|
Time
from admission to EVD placement (hours) |
Linear |
65.32
(-6.04-136.68) |
0.072 |
|
Time
from EVD placement to shunt (hours) |
Linear |
-50.21
(-208.70-108.28) |
0.530 |
|
Length
of stay (days) |
Linear |
10.53
(1.32-19.75) |
0.025* |
|
ICU length
of stay (days) |
Linear |
-1.13
(-7.18-12.74) |
0.808 |
RR:
Relative Risk; ß: Regression Coefficient; CI: Confidence Interval; EVD:
Extraventricular Drain; ICU: Intensive Care Unit.
Note: Model adjusted for age, sex, BMI,
smoking status, absence of a medical comorbidity, insurance status, and median
household income.
Reference
group: English-speaking
patients.
*p-value<0.05, **p-value<0.01.
3.4. Propensity Score Matched Analysis
All covariates demonstrated an SMD <0.2, ensuring that the propensity match created an equal distribution of covariates between SSPs and ESPs (Figure 1). A 1:3 propensity match was performed with a total of 64 patients included from the original sample (40.63% female, mean age: 50.77 ± 4.27 years). EVD placement continued to be higher in SSPs compared to ESPs (RR 1.62; 95% CI 1.12-2.35; p = 0.041; Figure 2). Additionally, time from admission to EVD was increased in SSPs compared to ESPs with a median difference of +9.00 hours (p = 0.037, Table 4). Complication rates, ICU admission, pain medication at discharge, and readmission were all statistically nonsignificant in the matched cohort (p > 0.3). Interestingly, LOS was lower for SSPs than ESPs in the matched cohort (11.50 vs 15.00 days), though this did not reach statistical significance (p = 0.460). Time from EVD placement to shunt procedure and ICU LOS were also nonsignificant (p > 0.1). Discharge disposition was also nonsignificant between SSPs and ESPs.
Table.
4. Results of
propensity-matched outcome comparisons between Spanish-speaking and
English-speaking patients who underwent a shunt placement for hydrocephalus.
|
Spanish (n=16) |
English (n=48) |
RR (95% CI) |
Median Difference |
p-value |
|
|
EVD Placement (%) |
81.25 |
50.00 |
1.62 (1.12-2.35) |
- |
0.041* |
|
Time from admission to EVD (hours, median, IQR) |
15.00 (5.00-24.00) |
6.0 0(3.00-12.50) |
- |
+9.00 |
0.037* |
|
Time from EVD to shunt (hours, median, IQR) |
316.00 (117.00-463.00) |
437.00 (293.00-624.00) |
- |
-121.00 |
0.089 |
|
LOS (days, median, IQR) |
11.50 (3.50-28.50) |
15.00 (4.00-26.25) |
- |
-3.50 |
0.464 |
|
ICU (%) |
43.75 |
33.33 |
1.31 (0.66-2.60) |
|
0.551 |
|
ICU LOS (days, median, IQR) |
15.00 (7.50-20.50) |
16.00 (6.00-22.00) |
- |
-1.00 |
0.484 |
|
Complications (%) |
25.00 |
25.00 |
1.00 (0.38-2.66) |
- |
1.000 |
|
Pain Medication at Discharge (%) |
62.50 |
75.00 |
0.83 (0.55-1.26) |
- |
0.352 |
|
Readmission within 30 Days of Discharge (%) |
12.50 |
22.92 |
0.55 (0.13-2.20) |
- |
0.489 |
|
Discharge Disposition (%) |
|
|
|
||
|
Home |
62.50 |
41.67 |
1.50 (0.90-2.49) |
- |
0.164 |
|
Hospice |
0.00 |
2.08 |
- |
- |
1.000 |
|
Acute Care Facility/In-Patient Rehabilitation |
25.00 |
29.17 |
0.86 (0.33-2.23) |
- |
1.000 |
|
SNF/Nursing Home |
6.25 |
10.42 |
0.60 (0.08-4.76) |
- |
1.000 |
|
Other |
6.25 |
16.67 |
0.38 (0.05-2.77) |
- |
0.430 |
Note: 1:3 propensity match adjusted for
age, sex, BMI, smoking status, absence of a medical comorbidity, insurance
status, and median household income.
EVD: Extraventricular Drain; IQR: Interquartile Range; LOS: Length of Stay; ICU: Intensive Care Unit; SNF: Skilled Nursing Facility. *p-value<0.05.
4. Discussion
This study evaluates and compares clinical outcomes between adult ESPs and SSPs undergoing shunt placement for hydrocephalus. We found that SSPs had significantly higher rates of EVD placement and ICU admission, as well as delayed EVD placement from admission, compared to ESPs. SSPs were also discharged less frequently with pain medications. Although initial LOS and ICU LOS were similar, adjusted analyses revealed significantly longer hospital stays for SSPs. Interestingly, SSPs had lower 30-day readmission rates. Complication rates were comparable between groups. These findings were partially confirmed in the propensity-matched cohort, which showed continued disparities in EVD placement and time to intervention.
Of note, following propensity matching, statistical significance was eliminated within our cohort for select variables. Moreover, the previously established increased LOS seen in SSPs compared to ESPs was reversed following matching, though this did not reach significance. This may be due in part to the decreased sample size following matching, minimizing statistical power. Nevertheless, these findings may suggest that the differences seen in the SSP population within our cohort are likely influenced more strongly by the disparity in baseline socioeconomic factors and less likely due to the language disparity itself. Despite not reaching statistical significance in all variables, the trends seen in our previous analysis persisted. This suggests that language may still be an independent predictor of the disparity in outcomes between SSPs and ESPs and warrants additional investigation with larger samples and prospective studies.
These findings build on prior work demonstrating that patients with LEP are at increased risk for adverse outcomes across surgical disciplines [22-24]. Moreover, a recent large study reported decreased readmissions among non-ESPs following surgery, consistent with our findings [25]. As proposed by those authors, and cautiously echoed here, this paradox may reflect multifactorial influences such as differences in care-seeking behaviors due to cultural beliefs, limited access to professional interpretation services, or misunderstandings arising from language-discordant discharge instructions.
In the context of hydrocephalus, where timely symptom recognition and intervention are critical, language barriers may lead to delayed presentation and more severe disease at admission. The higher rate of EVD placement and ICU admission among our SSPs supports this notion and is consistent with patterns seen in other emergent neurosurgical conditions [24]. Several systemic issues, such as language barriers, cultural differences, and lower health literacy may contribute to overall lower access to healthcare and thus, delayed presentation for SSPs in general [26-29]. To improve clinical outcomes for SSPs, we propose the following intervention to address the current health disparities faced by this population.
4.1. Development of Culturally and Linguistically Appropriate Patient Education Materials
Health literacy is a key determinant of timely care-seeking behavior [30, 31]. Providing Spanish-language educational resources on hydrocephalus may empower SSPs to recognize symptoms earlier and engage in their care more effectively. Patient education materials have been shown previously to improve clinical outcomes in neurosurgery regarding spinal surgery, specifically in increasing patient knowledge, reducing emergency department usage, and improving physical function following surgery [32-34]. Despite this, information regarding the current availability and readability of patient education materials concerning hydrocephalus remains limited. Moreover, even if patient education materials are available pertaining to hydrocephalus, this does not guarantee that they will be made available in an easy-to-understand Spanish version. For example, a previous study regarding the readability and availability of online information regarding spinal cord injury in Spanish at academic neurosurgical programs across the United States demonstrated that most affiliated websites did not provide any educational materials in Spanish [35]. Thus, this represents an opportunity for intervention from the neurosurgical community to create and distribute high-quality patient education materials in Spanish regarding hydrocephalus and other common neurosurgical pathologies. Future research can be directed to determine the best methods to increase education and community outreach to improve awareness of hydrocephalus within this community.
4.2. Cultural Competency and Humility Training (CCHT)
CCHT has been shown to be particularly effective in addressing disparities in pain control between SSPs and ESPs [36]. Studies have demonstrated that LEP patients are less likely to receive equivalent pain medications compared to their English-proficient counterparts in other postoperative settings [37, 38]. Disparities in pain control among SSPs have been hypothesized to be due to language barriers, diverse cultural perceptions regarding pain, differences in communicating pain to the healthcare team, or discrimination against SSPs [39, 40]. In the setting of shunt placement for hydrocephalus, adequate pain control is essential for optimal recovery [41, 42]. As such, neurosurgeons should seek to implement CCHT in their institutions locally, as well as promote its use more broadly to improve pain control for postoperative neurosurgical patients.
4.3. Expansion and Optimization of Medical Interpretation Services
Proper use of professional interpreters and bilingual providers is associated with improved clinical outcomes [43]. Despite guidelines, interpreter use remains inconsistent, particularly in high-acuity settings where staff may rely on ad hoc interpreters, such as family members, despite current evidence that this delivers suboptimal care [44-50]. In our study, ad hoc interpreters were used in approximately 15.6% of cases, and interpretation status was undocumented in 34.4%. These findings highlight both inconsistent utilization of formal interpretation services and suboptimal documentation, limiting our ability to determine whether observed disparities stem from interpreter access, underdocumentation, or broader structural issues.
To address these gaps, institutions should prioritize hiring certified interpreters, ensuring their availability across all shifts, and training clinical staff on appropriate and timely interpreter use. For complex or emergent neurosurgical care, in-person interpretation is preferred over telephone or video methods when feasible [51, 52]. Neurosurgeons can play a critical role by advocating for expanded interpreter services in high-need areas and encourage the training of all clinicians on interprofessional collaboration with certified medical interpreters to improve the quality of interpretation [53]. Furthermore, neurosurgical teams can lead efforts to standardize documentation of interpretation services, thereby enhancing transparency, continuity of care, and the quality of future research on language-based disparities.
4.4. Limitations and Future Directions
This study has potential limitations. One of the main limitations of this study is the small sample size of SSPs. This limited representation may affect the generalizability of our findings, potentially skewing the results and limiting the study’s applicability. Another significant limitation is the reliance on electronic medical records, where the language preference of patients was not always accurately reported or marked as Spanish. This could have resulted in an incorrect estimation of the number of SSPs, further contributing to the small sample size and affecting the reliability of our conclusions. These limitations should be considered when interpreting the results and planning future research to ensure more comprehensive and representative data.
5. Conclusion
This study highlights significant disparities in clinical outcomes between SSPs and ESPs undergoing shunt placement for hydrocephalus. SSPs were more likely to experience longer hospital stays, increased ICU utilization, higher rates of EVD placement, and reduced pain management at discharge. These differences underscore the need to address structural and communication barriers that affect SSPs in neurosurgical care. To reduce these disparities, we propose targeted interventions including the development of culturally appropriate education materials, cultural humility training for clinicians, and improved access to professional interpretation. Implementation of these strategies can improve patient-centered outcomes and promote equity across language groups. Efforts to address these disparities must be embedded in clinical practice, research, and policy to ensure all patients receive high-quality, equitable neurosurgical care regardless of their language proficiency or cultural background.
Data Availability
The data that support the findings of this study were collected from patient medical records, de-identified, and stored in a secure, institutional REDCap database. Due to the nature of this retrospective study and institutional privacy regulations, the data are not publicly available. However, de-identified data may be made available from the corresponding author upon reasonable request and with appropriate institutional approvals.
Conflicts of Interest
None.
Funding
None.
Ethical Approval
This study was approved by the University of Arizona Institutional Review Board as part of STUDY00002777.
Consent
Given the retrospective nature of this study, patient consent was waived by the Institutional Review Board prior to initiation of the study.
Author Contributions
Jacob A Saunders: Study conception and design, data collection, data analysis and interpretation, and manuscript writing. Mitchel L. Nelson: Data collection and manuscript writing. Scotty R. Wynn: Data collection and manuscript writing. Sussanah Colwey-Rallison: Data collection and manuscript writing. Ritu Bhalerao: Data collection. Valentyna Larchenko: Data collection and manuscript writing. Annie Pico: Study conception and design and data collection. Caominh Le: Study conception and design and data analysis. Kristin Nosova: Manuscript writing. Robert W. Bina: Manuscript writing.
Guarantor
Robert W. Bina.
REFERENCES
[1] Harold L Rekate “A contemporary
definition and classification of hydrocephalus.” Semin Pediatr Neurol,
vol. 16, no. 1, pp. 9-15, 2009. View at: Publisher Site | PubMed
[2] Miroslava Koleva; Orlando De Jesus
“Hydrocephalus.” In: StatPearls. Treasure Island (FL): StatPearls
Publishing; August 23, 2023. View at: PubMed
[3] Sukriti Das, Nicola Montemurro,
Musannah Ashfaq, et al. “Resolution of Papilledema Following
Ventriculoperitoneal Shunt or Endoscopic Third Ventriculostomy for Obstructive
Hydrocephalus: A Pilot Study.” Medicina (Kaunas), vol. 58, no. 2, pp.
281, 2022. View at: Publisher
Site | PubMed
[4] Neel H Mehta, Ana B W Greenberg ,
Kristopher T Kahle “The Efficacy of Endoscopic Third Ventriculostomy for
Idiopathic Normal Pressure Hydrocephalus.” World Neurosurg, vol. 179,
pp. 158-166, 2023. View at: Publisher
Site | PubMed
[5] Sarah Stricker, Raphael Guzman,
Thomas Blauwblomme, et al. “Is the Choroid Plexus Needed?” Pediatr Neurosurg,
vol. 57, no. 5, pp. 301-305, 2022. View at: Publisher Site | PubMed
[6] Frank J Attenello, Alvin Ng, Timothy
Wen, et al. “Racial and socioeconomic disparities in outcomes following
pediatric cerebrospinal fluid shunt procedures.” J Neurosurg Pediatr,
vol. 15, no. 6, pp. 560-566, 2015. View at: Publisher Site | PubMed
[7] Corey T Walker, Jonathan J Stone,
Minal Jain, et al. “The effects of socioeconomic status and race on pediatric
neurosurgical shunting.” Childs Nerv Syst, vol. 30, no. 1, pp. 117-122,
2014. View at: Publisher
Site | PubMed
[8] Gabriela D Ruiz Colón, Rebecca J
Pizzitola, Gerald A Grant, et al. “Disparities in Postoperative Communication
Patterns Among Spanish-speaking Pediatric Patients with Hydrocephalus.” J
Pediatr, vol. 263, pp. 113678, 2023. View at: Publisher Site | PubMed
[9] Sara Iglesias, Bienvenido Ros, Álvaro
Martín, et al. “Functional outcome in pediatric hydrocephalus: results of
applying the Spanish version of the Hydrocephalus Outcome Questionnaire.” J
Neurosurg Pediatr, vol. 21, no. 3, pp. 224-235, 2018. View at: Publisher Site | PubMed
[10] Ángela Ros-Sanjuán, Sara
Iglesias-Moroño, Bienvenido Ros-López, et al. “Quality of life in children with
hydrocephalus treated with endoscopic third ventriculostomy.” J Neurosurg
Pediatr, vol. 27, no. 5, pp. 503-510, 2021. View at: Publisher Site | PubMed
[11] Sara Iglesias, Bienvenido Ros, Angela
Ros, et al. “Quality of life in school-age children with shunt implantation due
to neonatal posthemorrhagic hydrocephalus.” Childs Nerv Syst, vol. 37,
no. 4, pp. 1127-1135, 2021. View at: Publisher Site | PubMed
[12] QuickFacts: United States. Census
Bureau QuickFacts. Published 2024. Accessed January 7, 2025.
[13] US Census Bureau. Overview of Race
and Hispanic Origin: 2010. Census.gov. Published October 2018.
[14] States U. Explore Census Data.
Census.gov. Published 2025. Accessed January 7, 2025.
[15] Luis E Escobedo, Lilia Cervantes,
Edward Havranek “Barriers in Healthcare for Latinx Patients with Limited
English Proficiency-a Narrative Review.” J Gen Intern Med, vol. 38, no.
5, pp. 1264-1271, 2023. View at: Publisher Site | PubMed
[16] Elisabeth Welty, Valerie A Yeager,
Claude Ouimet, et al. “Patient satisfaction among Spanish-speaking patients in
a public health setting.” J Healthc Qual, vol. 34, no. 5, pp. 31-38,
2012. View at: Publisher
Site | PubMed
[17] O Carrasquillo, E J Orav, T A
Brennan, et al. “Impact of language barriers on patient satisfaction in an
emergency department.” J Gen Intern Med, vol. 14, no. 2, pp. 82-87,
1999. View at: Publisher
Site | PubMed
[18] Betty M Luan-Erfe, J Mark Erfe, Bruno
DeCaria, et al. “Limited English Proficiency and Perioperative Patient-Centered
Outcomes: A Systematic Review.” Anesth Analg, vol. 136, no. 6, pp.
1096-1106, 2023. View at: Publisher
Site | PubMed
[19] Paul A Harris, Robert Taylor, Brenda
L Minor, et al. “The REDCap consortium: Building an international community of
software platform partners.” J Biomed Inform, vol. 95, pp. 103208, 2019.
View at: Publisher
Site | PubMed
[20] Paul A Harris, Robert Taylor, Robert
Thielke, et al. “Research electronic data capture (REDCap)--a metadata-driven
methodology and workflow process for providing translational research
informatics support.” J Biomed Inform, vol. 42, no. 2, pp. 377-381,
2009. View at: Publisher
Site | PubMed
[21] United States Census Bureau. Explore
Census Data. Data.census.gov. Published 2020.
[22] Betty M Luan-Erfe, J Mark Erfe, Bruno
DeCaria, et al. “Limited English Proficiency and Perioperative Patient-Centered
Outcomes: A Systematic Review.” Anesth Analg, vol. 136, no. 6, pp.
1096-1106, 2023. View at: Publisher
Site | PubMed
[23] Hyundeok Joo, Alicia Fernández,
Elizabeth C Wick, et al. “Association of Language Barriers With Perioperative
and Surgical Outcomes: A Systematic Review.” JAMA Netw Open, vol. 6, no.
7, pp. e2322743, 2023. View at: Publisher
Site | PubMed
[24] Gabriela D Ruiz Colón, Maria Isabel
Barros Guinle, Adela Wu, et al. “Neurosurgical Outcomes Among Non-English
Speakers: A Systematic Review and a Framework for Future Research.” World
Neurosurg, vol. 185, pp. 338-350.e1, 2024. View at: Publisher Site | PubMed
[25] Mariah
B Blegen, David S Zingmond, Nicholas J Jackson, et al. “Association of non-English
language preference with postoperative hospital visits among California Medicaid
enrollees.” Surgery, vol. 176, no. 6, pp. 1711-1720, 2024. View at: Publisher Site | PubMed
[26] Paul M Schyve “Language differences
as a barrier to quality and safety in health care: the Joint Commission
perspective.” J Gen Intern Med, vol. 22 Suppl 2, no. Suppl 2, pp.
360-361, 2007. View at: Publisher
Site | PubMed
[27] Jane H Brice, Debbie Travers,
Christopher S Cowden, et al. “Health literacy among Spanish-speaking patients
in the emergency department.” J Natl Med Assoc, vol. 100, no. 11, pp.
1326-1332, 2008. View at: Publisher Site | PubMed
[28] Andrew R Blundell, Daniela
Kroshinsky, Elena B Hawryluk, et al. “Disparities in telemedicine access for
Spanish-speaking patients during the COVID-19 crisis.” Pediatr Dermatol,
vol. 38, no. 4, pp. 947-949, 2021. View at: Publisher Site | PubMed
[29] Ferdinand Velasco, Donghan M Yang,
Minzhe Zhang, et al. “Association of Healthcare Access With Intensive Care Unit
Utilization and Mortality in Patients of Hispanic Ethnicity Hospitalized With
COVID-19.” J Hosp Med, vol. 16, no. 11, pp. 659-666, 2021. View at: Publisher Site | PubMed
[30] Mehmet Akif Erişen “Effect of Health Literacy and Patient
Activation on Health-Seeking Behaviour: A Cross-Sectional Study in Turkey.” Health Expect, vol. 27, no.
5, pp. e70052,2024. View at: Publisher
Site | PubMed
[31] Nancy D Berkman, Stacey L Sheridan,
Katrina E Donahue, et al. “Low health literacy and health outcomes: an updated
systematic review.” Ann Intern Med, vol. 155, no. 2, pp. 97-107, 2011.
View at: Publisher
Site | PubMed
[32] Alis J Dicpinigaitis, Boyi Li,
Jonathan Ogulnick, et al. “Evaluating the Impact of Neurosurgical Educational
Interventions on Patient Knowledge and Satisfaction: A Systematic Review of the
Literature.” World Neurosurg, vol. 147, pp. 70-78, 2021. View at: Publisher Site | PubMed
[33] Donna Eastwood, Neil Manson, Erin
Bigney, et al. “Improving postoperative patient reported benefits and
satisfaction following spinal fusion with a single preoperative education
session.” Spine J, vol. 19, no. 5, pp. 840-845, 2019. View at: Publisher Site | PubMed
[34] Eva Huysmans, Lisa Goudman, Iris
Coppieters, et al. “Effect of perioperative pain neuroscience education in
people undergoing surgery for lumbar radiculopathy: a multicentre randomised
controlled trial.” Br J Anaesth, vol. 131, no. 3, pp. 572-585, 2023.
View at: Publisher
Site | PubMed
[35] Jacques Lara-Reyna, Jorge A Roa, Kurt
A Yaeger, et al. “Availability and Readability of Spinal Cord Injury Online
Information Materials for Spanish Speaking Population in Neurosurgical Academic
Programs: A Nationwide Study.” Int J Spine Surg, vol. 15, no. 5, pp.
1039-1045, 2021. View at: Publisher
Site | PubMed
[36] Roberto Mora, Mervyn Maze “The role
of cultural competency training to address health disparities in surgical
settings.” Br Med Bull, vol. 150, no. 1, pp. 42-59, 2024. View at: Publisher Site | PubMed
[37] Hope E M Schwartz, Zachary A Matthay,
Rebecca Menza, et al. “Inequity in discharge pain management for trauma
patients with limited English proficiency.” J Trauma Acute Care Surg,
vol. 91, no. 5, pp. 898-902, 2021. View at: Publisher Site | PubMed
[38] Jana M Mossey “Defining racial and
ethnic disparities in pain management.” Clin Orthop Relat Res, vol. 469,
no. 7, pp. 1859-1870, 2011. View at: Publisher Site | PubMed
[39] Rachel A Levy, Allison H Kay, Nancy
Hills, et al. “Exploring the relationship between language, postoperative pain,
and opioid use.” AJOG Glob Rep, vol. 4, no. 2, pp. 100342, 2024. View
at: Publisher
Site | PubMed
[40] Calia A Torres, Beverly E Thorn,
Shweta Kapoor, et al. “An Examination of Cultural Values and Pain Management in
Foreign-Born Spanish-Speaking Hispanics Seeking Care at a Federally Qualified
Health Center.” Pain Med, vol. 18, no. 11, pp. 2058-2069, 2017. View at:
Publisher Site | PubMed
[41] Kerry-Ann S Mitchell, Ian Zelko,
Tamir Shay, et al. “The Impact of Hydrocephalus Shunt Devices on Quality of
Life.” J Craniofac Surg, vol. 32, no. 5, pp. 1746-1750, 2021. View at: Publisher Site | PubMed
[42] Harold L Rekate, Dory Kranz
“Headaches in patients with shunts.” Semin Pediatr Neurol, vol. 16, no. 1, pp.
27-30, 2009. View at: Publisher
Site | PubMed
[43] Daniel M Seible, Souma Kundu, Alexa
Azuara, et al. “The Influence of Patient-Provider Language Concordance in
Cancer Care: Results of the Hispanic Outcomes by Language Approach (HOLA)
Randomized Trial.” Int J Radiat Oncol Biol Phys, vol. 111, no. 4, pp.
856-864, 2021. View at: Publisher
Site | PubMed
[44] D W Baker, R M Parker, M V Williams,
et al. “Use and effectiveness of interpreters in an emergency department.” JAMA,
vol. 275, no. 10, pp. 783-788, 1996. View at: PubMed
[45] Sonja C Burbano O'Leary, Steven
Federico, Louis C Hampers “The truth about language barriers: one residency
program's experience.” Pediatrics, vol. 111, no. 5 Pt 1, pp. e569-e573,
2003. View at: Publisher
Site | PubMed
[46] Karen C Lee, Jonathan P Winickoff,
Minah K Kim, et al. “Resident physicians' use of professional and
nonprofessional interpreters: a national survey.” JAMA, vol. 296, no. 9,
pp. 1050-1053, 2006. View at: Publisher
Site | PubMed
[47] Lenny López, Fátima Rodriguez, Diego
Huerta, et al. “Use of interpreters by physicians for hospitalized limited
English proficient patients and its impact on patient outcomes.” J Gen
Intern Med, vol. 30, no. 6, pp. 783-789, 2015. View at: Publisher Site | PubMed
[48] Yael Schenker, Eliseo J Pérez-Stable,
Dana Nickleach, et al. “Patterns of interpreter use for hospitalized patients
with limited English proficiency. J Gen Intern Med, vol. 26, no. 7, pp.
712-717, 2011. View at: Publisher
Site | PubMed
[49] Gregory Juckett, Kendra Unger
“Appropriate use of medical interpreters.” Am Fam Physician, vol. 90,
no. 7, pp. 476-480, 2014. View at: PubMed
[50] Glenn Flores, Milagros Abreu, Cara
Pizzo Barone, et al. “Errors of medical interpretation and their potential
clinical consequences: a comparison of professional versus ad hoc versus no
interpreters.” Ann Emerg Med, vol. 60, no. 5, pp. 545-553, 2012. View
at: Publisher
Site | PubMed
[51] Nicholas V Nguyen, Andres H Guillen
Lozoya, Maria A Caruso, et al. “Through the eyes of Spanish-speaking patients,
caregivers, and community leaders: a qualitative study on the in-patient
hospital experience.” Int J Equity Health, vol. 23, no. 1, pp. 164,
2024. View at: Publisher
Site | PubMed
[52] K Casey Lion, Julie C Brown, Beth E
Ebel, et al. “Effect of Telephone vs Video Interpretation on Parent
Comprehension, Communication, and Utilization in the Pediatric Emergency
Department: A Randomized Clinical Trial.” JAMA Pediatr, vol. 169, no.
12, pp. 1117-1125, 2015. View at: Publisher Site | PubMed
[53] Daniela M Gomez Zubieta, Evelyn Londono, Alisha Heximer, et al. “Examining Interpreter Services to Better Characterize Areas for Quality Improvement.” J Surg Res, vol. 304, pp. 246-251, 2024. View at: Publisher Site | PubMed