Received: Sun 03, Aug 2025
Accepted: Fri 22, Aug 2025
Abstract
Background: Cystic lesions containing colorless, transparent cerebrospinal fluid are typically classified as arachnoid cysts, which most commonly occur in the middle cranial fossa and cerebellopontine angle region. However, cysts originating from the pituitary stalk are exceptionally rare. To date, no relevant cases have been reported in the international literature.
Case Description: A 58-year-old female patient presented to our hospital with complaints of headache, dizziness, and visual deterioration. Magnetic resonance imaging (MRI) revealed an intrasellar-suprasellar cystic lesion measuring approximately 2.2×1.8×1.7 cm3, with no calcification or significant enhancement. The differential diagnosis included pituitary stalk cyst versus pituitary adenoma. The patient underwent craniotomy via a subfrontal approach, during which the tension triangle of anterior cranial base was opened, revealing complete cystic degeneration of the pituitary stalk. Comprehensive fenestration of both anterior and posterior cyst walls was then performed. The postoperative course was uneventful, with no new neurological deficits or endocrine dysfunction.
Conclusion: This case represents the first reported craniotomy for a pituitary stalk cyst, where complete fenestration of both cyst walls was achieved via the first interoptic space to preserve the pituitary stalk's integrity. Furthermore, we propose the novel concept of the tension triangle of anterior cranial base, elucidates the methodological approach to achieving the modern neurosurgical principle of "maximizing lesion resection while preserving functional integrity".
Keywords
Pituitary stalk cyst, subfrontal approach, tension triangle of anterior cranial base, cyst fenestration, functional preservation
1. Introduction
Pituitary stalk lesions constitute a rare entity in neurosurgical practice. Although existing literature has described the surgical management of pituitary stalk epidermoid cysts via either transcranial or endoscopic approaches [1-3], reports of isolated pituitary stalk cysts (PSCs) remain exceptionally scarce [4, 5]. Given the pituitary stalk's intimate anatomical relationship with both the hypothalamic-pituitary axis and visual pathways - wherein lesions like pituitary adenomas and craniopharyngiomas typically manifest as endocrine dysfunction or visual impairment - managing pure cystic lesions requires particularly meticulous preservation of structural and functional integrity. Although minimally invasive, the transnasal endoscopic approach entails elevated risks of stalk injury and cerebrospinal fluid leakage and olfactory impairment due to anatomically constrained working space [6-8]. Currently, no consensus treatment protocols for PSCs exist in published literature. We present a successfully treated case of isolated pituitary stalk cyst (PSC) via a subfrontal approach with complete fenestration through the interoptic space with opening the tension triangle of anterior cranial base, supplemented by comprehensive anatomical analysis and surgical strategy discussion, thereby offering valuable clinical reference for similar cases.
2. Clinical History and Physical Examination
A 58-year-old female was admitted to our hospital with complaints of headache, dizziness and visual impairment. Physical examination in the outpatient department revealed a visual acuity of 0.4 in both eyes. CT scan demonstrated a hypodense occupying lesion in the sellar region with progressive visual deterioration. The patient denied polyuria or polydipsia and maintained normal mental status and appetite.
3. Laboratory Tests
It revealed mild elevation of her prolactin level to 81.16 ng/mL with a cortisol level of 481 nmol/L, while thyroid function tests showed no significant abnormalities. Routine blood tests including complete blood count, biochemical profile and coagulation studies were all within normal limits.
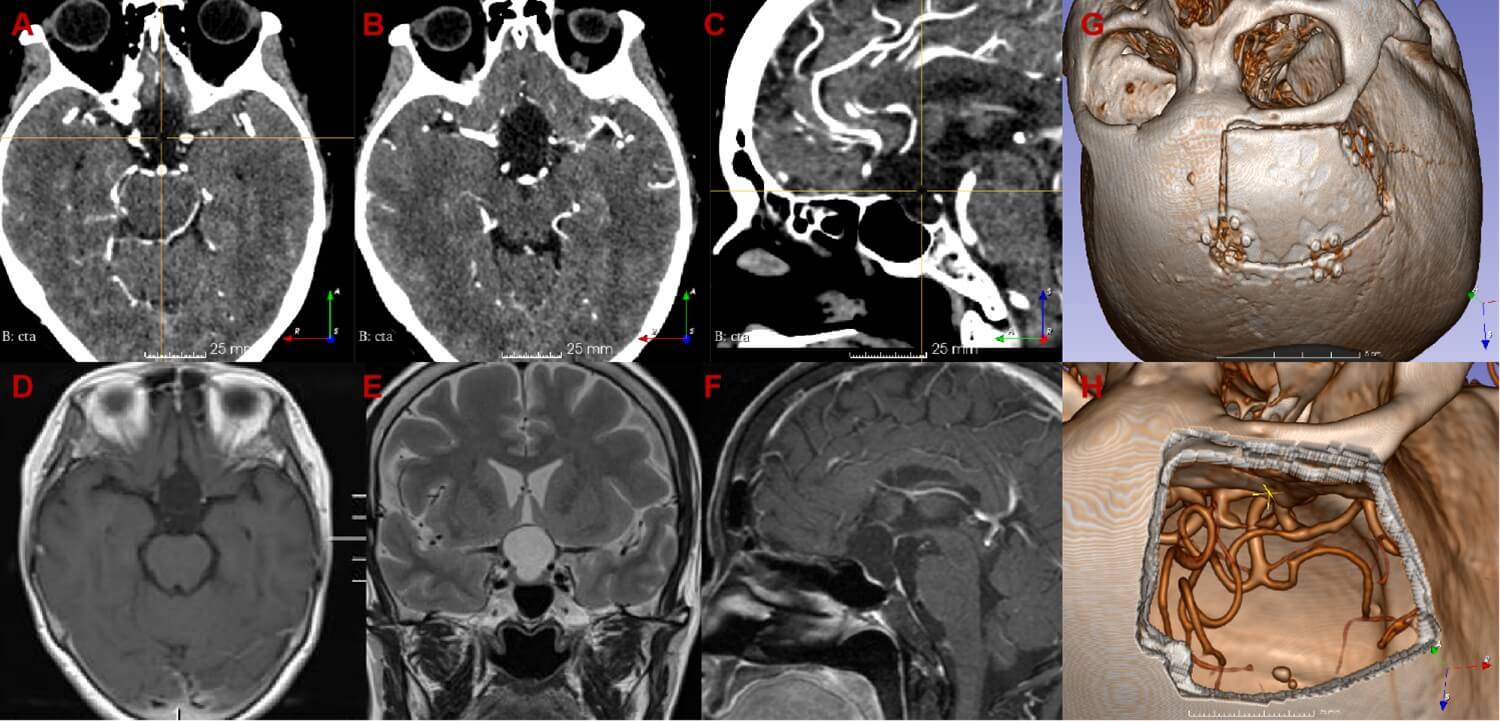
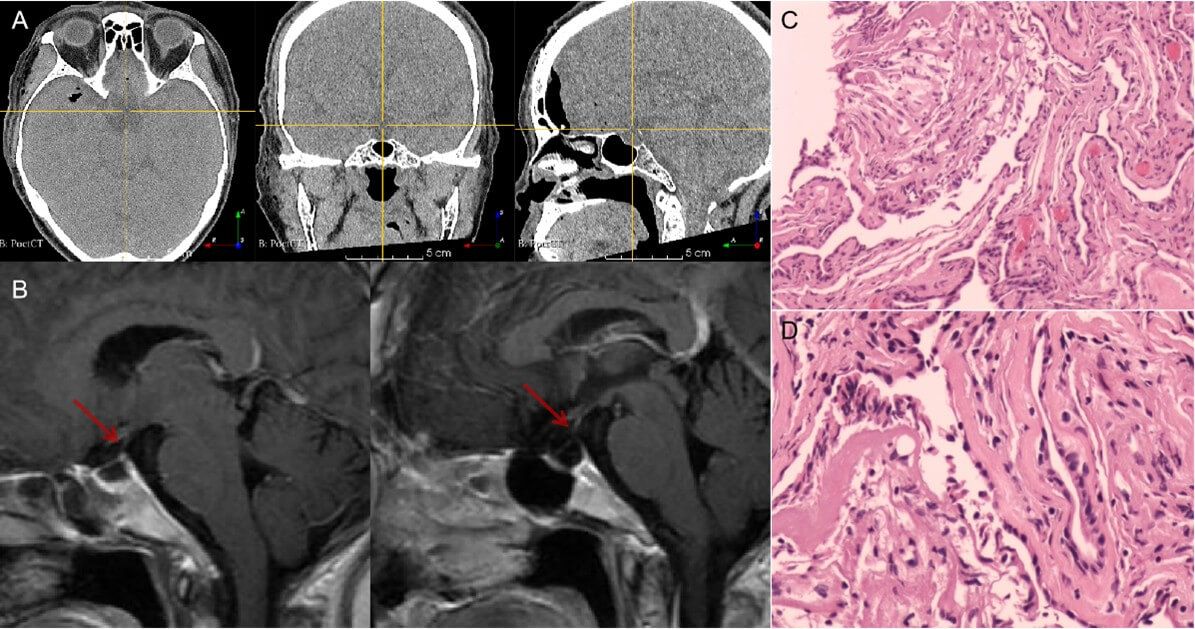
4. Imaging Findings (Figure 1)
CT revealed a hypodense lesion without calcification. CTA demonstrated the lesion's close proximity to the Circle of Willis. MRI identified an intrasellar-suprasellar cystic lesion measuring approximately 2.2×1.8×1.7 cm3, showing no significant enhancement. The pituitary gland was displaced anteriorly, with poor visualization of the pituitary stalk.
5. Differential Diagnosis
Pituitary stalk cyst versus pituitary adenoma.
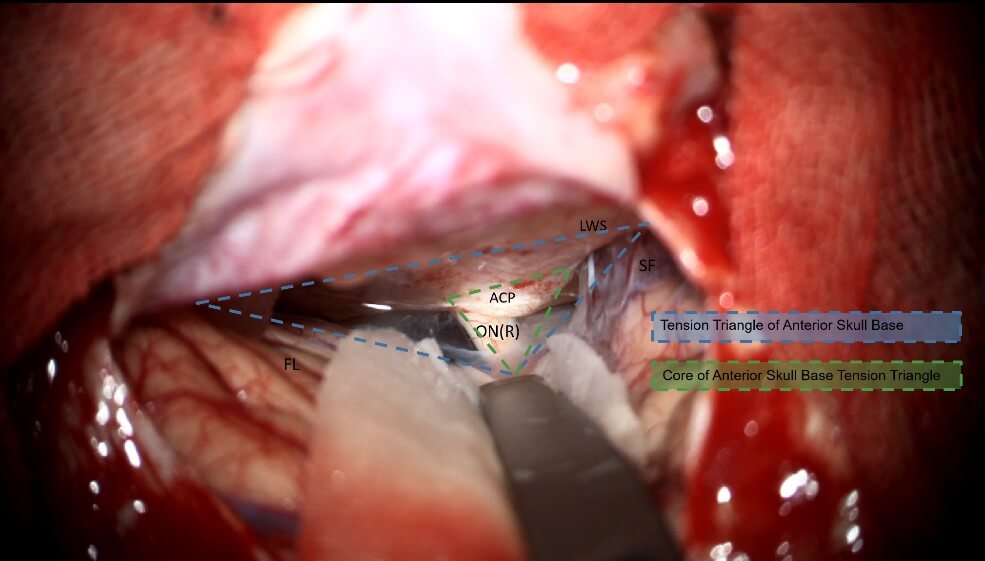
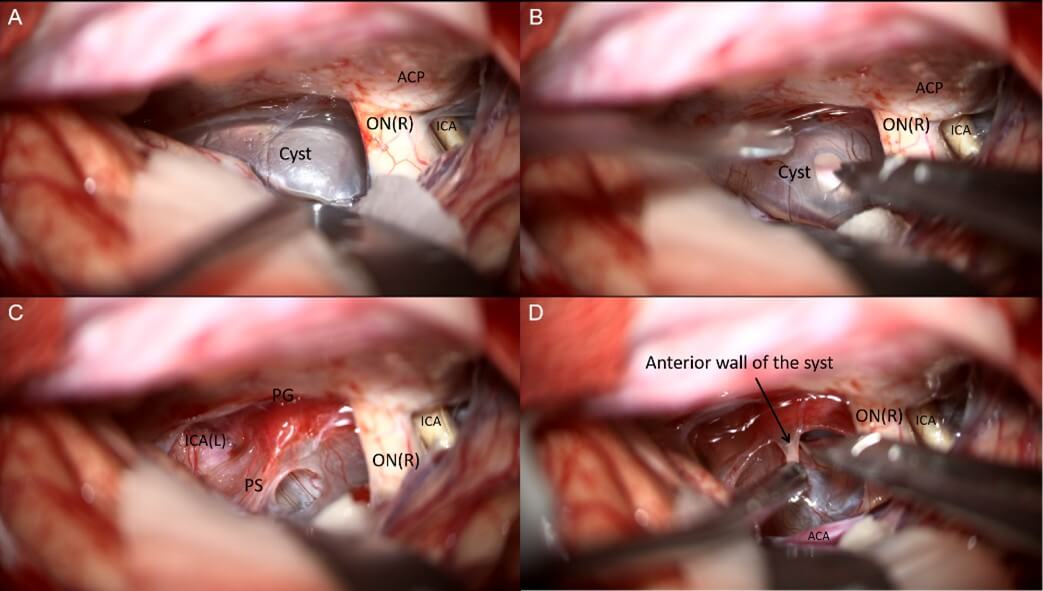
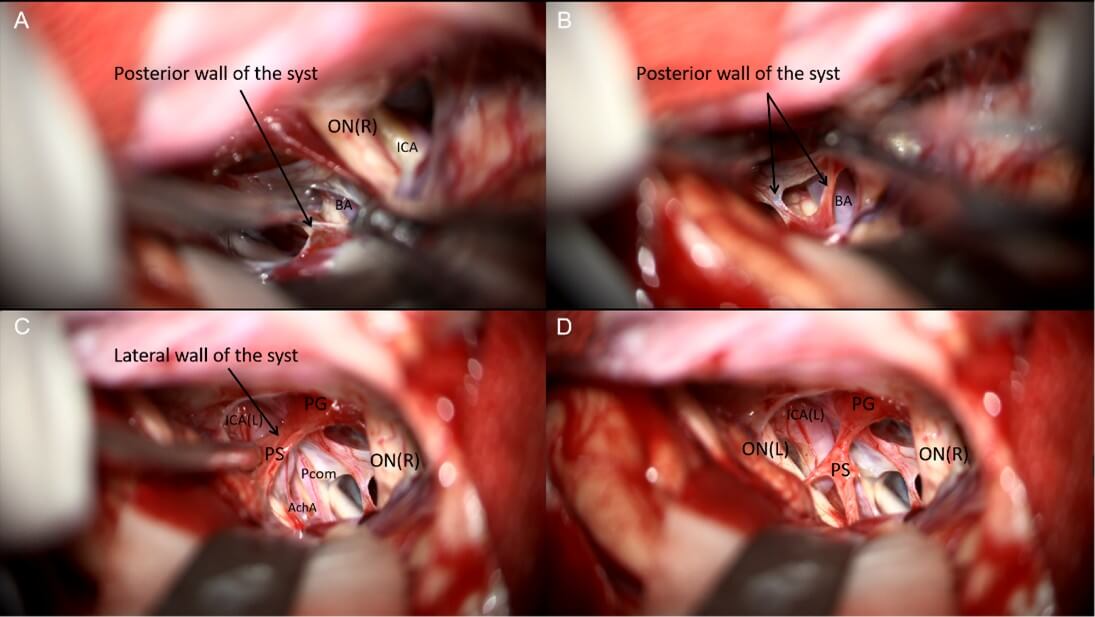
6. Operative Procedure (Figure 2-4 & Video 1)
A right subfrontal approach was performed. A frontotemporal skin flap and subfrontal craniotomy were created, followed by flattening of the anterior skull base. The dura was carefully reflected toward the frontal base, followed by sequential opening of the optic nerve cistern, carotid cistern, and sylvian cistern to access the tension triangle of anterior cranial base, allowing controlled cerebrospinal fluid (CSF) release. The arachnoid membranes around the optic nerves and chiasm were dissected. Upon exploration of the first interspace (the space between the bilateral optic nerves), a translucent, cystic lesion was identified with fine vascular networks on its surface. The cyst displaced the optic nerves and internal carotid arteries laterally, partially occupied the prepontine cistern posteriorly, compressed the optic chiasm superiorly, and extended into the sella inferiorly. The arachnoid adhesions between the cyst and the surrounding structures (optic nerves, chiasm, and internal carotid arteries) were meticulously dissected. No distinct pituitary stalk was initially visualized. A fenestration was made in the avascular region of the cyst’s anterior wall, releasing clear, colorless fluid and reducing the cyst’s tension. Upon decompression, a dark-red pituitary stalk became visible within the cyst wall. Further arachnoid dissection around the stalk was performed, followed by fenestration and partial resection of the cyst’s posterior avascular wall, exposing the proximal basilar artery in the prepontine cistern. Intrasellar exploration confirmed the pituitary gland’s anterior position. The pituitary stalk and hypothalamic structures were preserved intact, with no injury to the optic nerves or surrounding vessels. The procedure was concluded with watertight dural closure, obliteration of the frontal sinus, repositioning of the bone flap, and multilayer scalp suturing.
7. Clinical Outcomes (Figure 5)
The patient recovered uneventfully without postoperative complications such as fever or diabetes insipidus. The scalp incision healed well. Follow-up CT showed no surgical site hemorrhage, while MRI demonstrated complete resolution of the sellar cyst with preserved pituitary gland and stalk anatomy. Pathological examination confirmed the diagnosis of a benign cyst.
8. Literature Review
A systematic search of the PubMed database was conducted using the keywords "pituitary stalk cyst" and "craniotomy", which yielded no relevant published reports.
9. Discussion
The pituitary stalk, a delicate 2-3 mm structure composed of hypothalamic neuronal axons, portal vasculature and glial cells, serves as the crucial neuroendocrine conduit connecting the hypothalamus to the pituitary gland. This anatomically unique region's physiological significance necessitates specialized surgical considerations, as any operative injury may result in permanent diabetes insipidus, hypopituitarism or even more severe complications [9-11].
The main categories of pituitary stalk-related pathologies include tumors, inflammatory conditions, and developmental abnormalities. While most previously reported cases in the literature describe epidermoid cysts [1, 2, 5], isolated pituitary stalk cysts have not been documented. In this case, we successfully performed an anatomical fenestration of the pituitary stalk cyst wall via a subfrontal approach through the first interspace. This procedure not only completely preserved the pituitary stalk structure but also avoided postoperative complications such as diabetes insipidus, providing an important reference for the treatment of this rare condition.
The endoscopic endonasal approach for pituitary stalk lesions presents several technical difficulties that warrant careful consideration. First, the confined transsphenoidal working space makes it particularly challenging to adequately dissect cyst walls that extend into the suprasellar region. Second, the limited maneuverability of endoscopic instruments restricts multidirectional dissection capabilities, and the technical success heavily depends on the surgeon's individual skill level and experience and coordination due to the steep learning curve associated with this approach [12]. Most importantly, the inferior-to-superior viewing angle inherently positions both the pituitary gland and stalk directly in the surgical path, resulting in a substantially higher risk of pituitary stalk injury - literature reports indicate a 21.3-78.7% incidence of new-onset diabetes insipidus following such procedures [13-15]. Additionally, opening the sellar floor inevitably creates potential cerebrospinal fluid leakage, necessitating complex multilayer reconstruction [16]. In light of these considerable challenges, we determined that a transcranial approach would provide superior surgical access and better preservation of critical neurovascular structures in this particular case.
We selected the classic subfrontal approach due to its distinct advantages for this midline skull base lesion: First, it allows thorough arachnoid dissection around the carotid arteries, optic nerves and sylvian fissure with cerebrospinal fluid release, effectively reducing brain tension of whole anterior skull base. When combined with proper positioning, this technique minimizes frontal lobe retraction and potential injury [17]. Second, the cyst-expanded the interoptic space provides ample three-dimensional working room around the pituitary stalk, enabling multidirectional cyst dissection. When needed, opening the second space (optic-carotid cistern) can further improve exposure. Third, this approach offers direct visualization of the anterior circle of willis, permitting priority vascular control when necessary.
The recently developed endoscopic supraorbital keyhole technique, while offering clinical advantages such as minimal incisions and direct visual access, warrants careful consideration in this particular case [18-20]. Notably, our surgical strategy for this pituitary stalk-originating cyst prioritized complete fenestration over total resection. The conventional subfrontal approach demonstrated distinct superiority in managing this large (>2 cm) prepontine cistern-extending cyst, providing both enhanced operative space and superior vascular control - a perfect embodiment of the modern minimally invasive neurosurgical philosophy that emphasizes "simultaneous preservation of function and anatomical access". Moreover, we maintain that the dimensions of the scalp incision and bone flap do not equate to neural protection. Optimal brain relaxation constitutes the most effective neuroprotection strategy. These two principles are particularly crucial for skull base lesions adjacent to critical neurovascular structures, such as pituitary adenoma and craniopharyngioma in the sellar region.
10. Conclusion
This is a surgical report of a solitary pituitary stalk cyst treated via a subfrontal approach with fenestration of both anterior and posterior cyst walls. By releasing the tension triangle at the anterior skull base, ample operative space was achieved to preserve the pituitary stalk's structural and functional integrity. Compared to endoscopic endonasal surgery, this approach avoided CSF leakage and related complications. The surgical philosophy emphasizing maximal exposure with functional preservation proves particularly crucial for sellar and skull base lesions.
Data Availability
The raw data supporting this study cannot be made publicly available due to containing sensitive patient information and institutional policies. Processed imaging data and surgical schematics are provided in the Supplementary Materials. Requests for specific data points will be considered by the corresponding author following institutional review.
Conflicts of Interest
None.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 82270825) and the High talent project of Hunan Province (Grant No. 2022WZ1031) and the National Key Clinical Specialty Major Research Program(Grant No. 20230422).
Acknowledgments
First and foremost, we thank the patient for entrusting us with her care and consenting to educational use of her case. The nursing staff of Ward 35 in Xinagya hospital deserves particular recognition for their exceptional postoperative care. We acknowledge Professor Rhoton's pioneering work on pituitary stalk anatomy which informed our surgical approach, and the anonymous reviewers whose suggestions significantly improved this manuscript.
Ethical Approval
As a retrospective study, this research was granted exemption approval by the Ethics Committee of Xiangya Hospital, Central South University in accordance with exemption clauses for retrospective studies under the Declaration of Helsinki and China's Ethical Review Measures for Biomedical Research Involving Humans. All patient data were de-identified.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. The consent form specifically authorized: Use of clinical data and imaging materials for academic purposes Publication of surgical photographs and video recordings Potential online availability of supplementary materials A copy of the signed consent document is available for review by the Editor-in-Chief upon request.
Registration of Research Studies
This is a single retrospective case report that does not meet the criteria requiring study registration per the World Medical Association's Declaration of Helsinki 2013. The study was granted exemption from registration by the Ethics Committee of Xiangya Hospital, Central South University. All patient data—including clinical records, imaging studies, surgical photographs, and video recordings—were fully de-identified prior to analysis.
Guarantor
Prof. Xuejun Li as the guarantor takes ultimate responsibility for the study design, data integrity, and publication decisions.
Supplementary Materials
This article includes five supplementary figures (Figures S1-S5) and one surgical video (Video S1), which provide additional technical details and visual documentation of the procedure.
REFERENCES
[1] Paul
Lee, Khaled M Krisht, Perkins Mukunyadzi, et al. “Resection of an Isolated
Pituitary Stalk Epidermoid Cyst Through a Pretemporal Approach: Case Report and
Review of the Literature.” World Neurosurg, vol. 146, pp. 26-30, 2021.
View at: Publisher Site | PubMed
[2] Ana
C I Nakassa, Joseph D Chabot, Carl H Snyderman, et al. “Complete endoscopic
resection of a pituitary stalk epidermoid cyst using a combined infrasellar
interpituitary and suprasellar endonasal approach: case report.” J Neurosurg,
vol. 128, no. 2, pp. 437-443, 2018. View at: Publisher Site | PubMed
[3] Eduardo
de Arnaldo Silva Vellutini, Felix Hendrik Pahl, Aldo Eden Cassol Stamm, et al.
“Endoscopic resection of sellar and suprasellar epidermoid cyst: report of two
cases and review of literature.” Br J Neurosurg, vol. 38, no. 2, pp.
361-366, 2024. View at: Publisher Site | PubMed
[4] Demetra
Rupp, Mark Molitch “Pituitary stalk lesions.” Curr Opin Endocrinol Diabetes
Obes, vol. 15, no. 4, pp. 339-345, 2008. View at: Publisher Site | PubMed
[5] Jean-François Bonneville “Pituitary
Stalk Cysts.” In: Tricks and Traps in MRI of the Pituitary Region . Springer,
Cham 2024. View at: Publisher Site
[6] Varun
R Kshettry, Hyunwoo Do, Khaled Elshazly, et al. “The learning curve in
endoscopic endonasal resection of craniopharyngiomas.” Neurosurg Focus,
vol. 41, no. 6, pp. E9, 2016. View at: Publisher Site | PubMed
[7] Harisinh
Parmar, Hirotaka Hasegawa, Yuki Shinya, et al. “Contribution of watertight
dural closure to prevention of postoperative cerebrospinal fluid leakage in
endoscopic transnasal surgery for intradural lesions.” Neurosurg Focus,
vol. 58, no. 2, pp. E5, 2025. View at: Publisher Site | PubMed
[8] Jae
Yoon Lee, Jae Sung Park, Sin Soo Jeun, et al. “Sinonasal Complications of
Combined Transseptal-Transnasal and Bilateral Transnasal Approaches for
Endoscopic Endonasal Transsphenoidal Pituitary Surgery.” World Neurosurg,
vol. 192, pp. e410-e415, 2024. View at: Publisher Site | PubMed
[9] Roberto
Salvatori “Pituitary Stalk Lesions: Causes and Diagnostic Challenges.” Endocr
Pract, vol. 3, pp. S1530-891X(25)00902- S1530-891X(25)00904, 2025. View at:
Publisher Site | PubMed
[10] Aydin
Sav, Grazia Menna, Carlo Serra, et al. “Anatomy of the pituitary gland.” Best
Pract Res Clin Endocrinol Metab, vol. 39, no. 3, pp. 102013, 2025. View at:
Publisher Site | PubMed
[11] Benoit
Hudelist, Angela Elia, Alexandre Roux, et al. “Management and outcomes of
internal carotid artery, anterior cerebral artery, or middle cerebral artery
injury during microsurgical approach of the anterior and middle cranial skull
base: insights from a systematic review and a case series.” Neurosurg Rev,
vol. 48, pp. 67, 2025. View at: Publisher Site
[12]
Nicholas G Candy, Christopher
Ovenden, Alistair K Jukes, et al. “The learning curve for endoscopic endonasal
pituitary surgery: a systematic review.” Neurosurg Rev, vol. 46, no. 1,
pp. 241, 2023. View at: Publisher Site | PubMed
[13]
Amin B Kassam, Paul A Gardner, Carl H
Snyderman, et al. “Expanded endonasal approach, a fully endoscopic transnasal
approach for the resection of midline suprasellar craniopharyngiomas: a new
classification based on the infundibulum.” J Neurosurg, vol. 108, no. 4,
pp. 715-728, 2008. View at: Publisher Site | PubMed
[14]
M G Yaşargil, M Curcic, M Kis, et al. “Total
removal of craniopharyngiomas. Approaches and long-term results in 144
patients.” J Neurosurg, vol. 73, no. 1, pp. 3-11, 1990. View at: Publisher Site | PubMed
[15]
Rushikesh S Joshi, Matheus P Pereira,
Robert C Osorio, et al. “Identifying risk factors for postoperative diabetes
insipidus in more than 2500 patients undergoing transsphenoidal surgery: a
single-institution experience.” J Neurosurg, vol. 137, no. 3, pp.
647-657, 2022. View at: Publisher Site | PubMed
[16]
Bertrand Baussart, Alice Venier, Anne
Jouinot, et al. “Closure strategy for endoscopic pituitary surgery: Experience
from 3015 patients.” Front Oncol, vol. 12, pp. 1067312, 2023. View at: Publisher Site | PubMed
[17]
J Li, A W Gelb, A M Flexman, et al.
“Definition, evaluation, and management of brain relaxation during craniotomy.”
Br J Anaesth, vol. 116, no. 6, pp. 759-769, 2016. View at: Publisher
Site | PubMed
[18]
Bhanu Pratap Singh Chauhan, Ketan
Hedaoo, Vijay Parihar, et al. “Exoscopic Supraorbital Keyhole Approach for
Skull Base Lesions: An Institutional Experience.” Asian J Neurosurg,
vol. 20, no. 2, pp. 350-356, 2025. View at: Publisher Site | PubMed
[19]
Mehdi Khaleghi, Kyle C Wu, Daniel M
Prevedello “Fully Endoscopic Minimally Invasive Trans-Eyebrow Supraorbital
Translaminar Approach to Third Ventricle Craniopharyngiomas: Technical Nuances
and Stepwise Illustrative Description.” World Neurosurg, vol. 186, pp.
78-86, 2024. View at: Publisher Site | PubMed
[20] Tsuyoshi Sasaki, Hiroki Morisako, Masaki Ikegami, et al. “Endoscopic Supraorbital Eyebrow Approach for Medium-Sized Tuberculum Sellae Meningiomas: A Cadaveric Stepwise Dissection, Technical Nuances, and Surgical Outcomes.” World Neurosurg, vol. 176, pp. e40-e48, 2023. View at: Publisher Site | PubMed