Received: Tue 15, Jul 2025
Accepted: Mon 04, Aug 2025
Abstract
Tetrodotoxin poses significant threats to human life. Once poisoned, few people can survive. There is currently a lack of treatment guidelines for tetrodotoxin poisoning. This article presents a case study detailing the treatment and rehabilitation process of a patient who consumed a dosage of tetrodotoxin significantly exceeding the lethal threshold.
Keywords
Case report, tetrodotoxin, poisoning, treatment
1. Introduction
The incidence of puffer fish poisoning is rarely reported, and once it occurs, it has a great impact on life and quality of life. At present, the success rate of treatment is low, and the case reported in this article shows that after the patient ingests a lethal dose of tetrodotoxin, normal neurological function returns within a few days after the vital signs are stabilized, which is due to the treatment method and speed of the entire team. This case can provide treatment ideas for such patients. Tetrodotoxin poisoning predominantly originates from Asia, particularly in Japan, Thailand, and China, where there is a higher prevalence of poisoning incidents among elderly and male populations [1]. Despite the limited number of reported cases, statistical data suggests that the fatality rate of tetrodotoxin poisoning in Japan is estimated to be at least 60% [2].
Tetrodotoxin, a non-protein alkaloid toxin, possesses a chemically stable structure that remains unaffected by thermal and acidic conditions. Its mechanism of action involves the inhibition of sodium ion, thereby impeding the signaling process between nerves and muscles [3]. The lethal amount of tetrodotoxin is approximately 10 μg/kg, meaning that if an adult weighing 50 kg were to consume 0.5 mg of tetrodotoxin, it could result in the impairment of nerve conduction, leading to paralysis, respiratory failure, and ultimately, death [4]. The incubation period of poisoning is brief, as indicated by pertinent reports which suggest that symptoms may manifest within 10-30 minutes of poisoning, potentially leading to fatality within 4 hours [5]. Consequently, the prompt identification and treatment of such cases is of utmost importance. The subsequent account outlines the survival of a patient who ingested a significantly higher dosage of tetrodotoxin than the lethal threshold, serving as a clinical reference for treatment. Informed consent was obtained from the patient to disclose the details of this case.
2. General Information
Patient, a middle-aged and elderly men old, experienced perioral numbness and limb weakness 30 minutes after consuming the toxic substance on September 10, 2023. The patient experienced emesis once, expelling approximately 800 ml of gastric contents. Subsequently, the patient progressively deteriorated, resulting in limb immobility. In response to the severity of the situation, the patient's family promptly contacted the emergency center and was sent to the emergency room of Qinhuangdao Traditional Chinese Medicine Hospital for urgent medical intervention. The subsequent medical evaluation revealed the following findings: blood pressure of 198/95 mmHg, arterial blood gas analysis indicating a pH of 7.14, carbon dioxide partial pressure of 79.9 mmHg, oxygen partial pressure of 84 mmHg, lactate level of 6.3 mmol/L, and creatine kinase level of 316 U/L.
3. Treatment
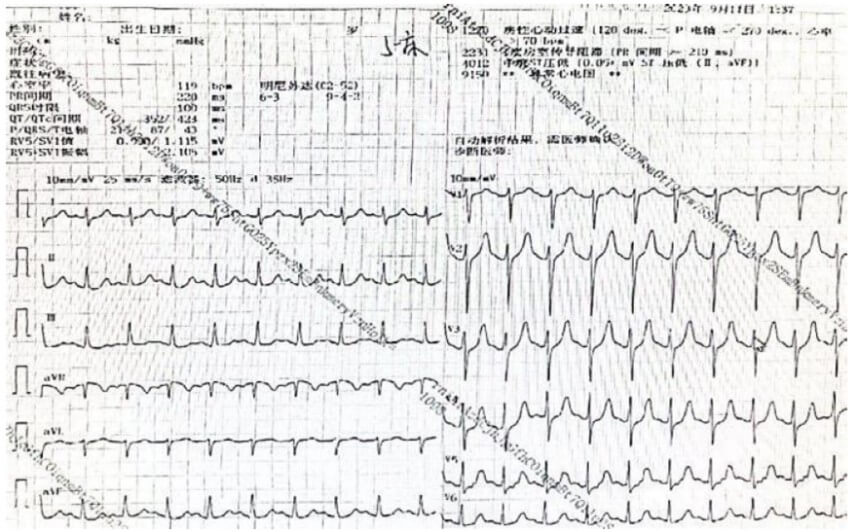
After admission, the patient immediately underwent gastric lavage. During treatment, the patient developed unconsciousness, stoppage of breathing, decreased blood oxygen, and stopped heartbeat. Tracheal intubation and connection to respirator, cardiopulmonary resuscitation, and Epinephrine boosting therapy were administered. After 6 minutes, the patient's heart rate recovered and 125 ml of Sodium Bicarbonate was administered intravenously to induce systemic alkalinization. 1 mg of Atropine and 10 mg of Dexamethasone were administered intravenously to counteract striated muscle inhibition and detoxification. The patient's physical signs remain stable, consciousness is unclear, temperature is 36.0 °C, heart rate is 138 beats per minute, blood pressure is 120/81 mmHg, and breathing is assisted by a respirator. The light reflex of both pupils disappears, and the respiratory sounds in both lungs are weak. The electrocardiogram is shown in (Figure 1).
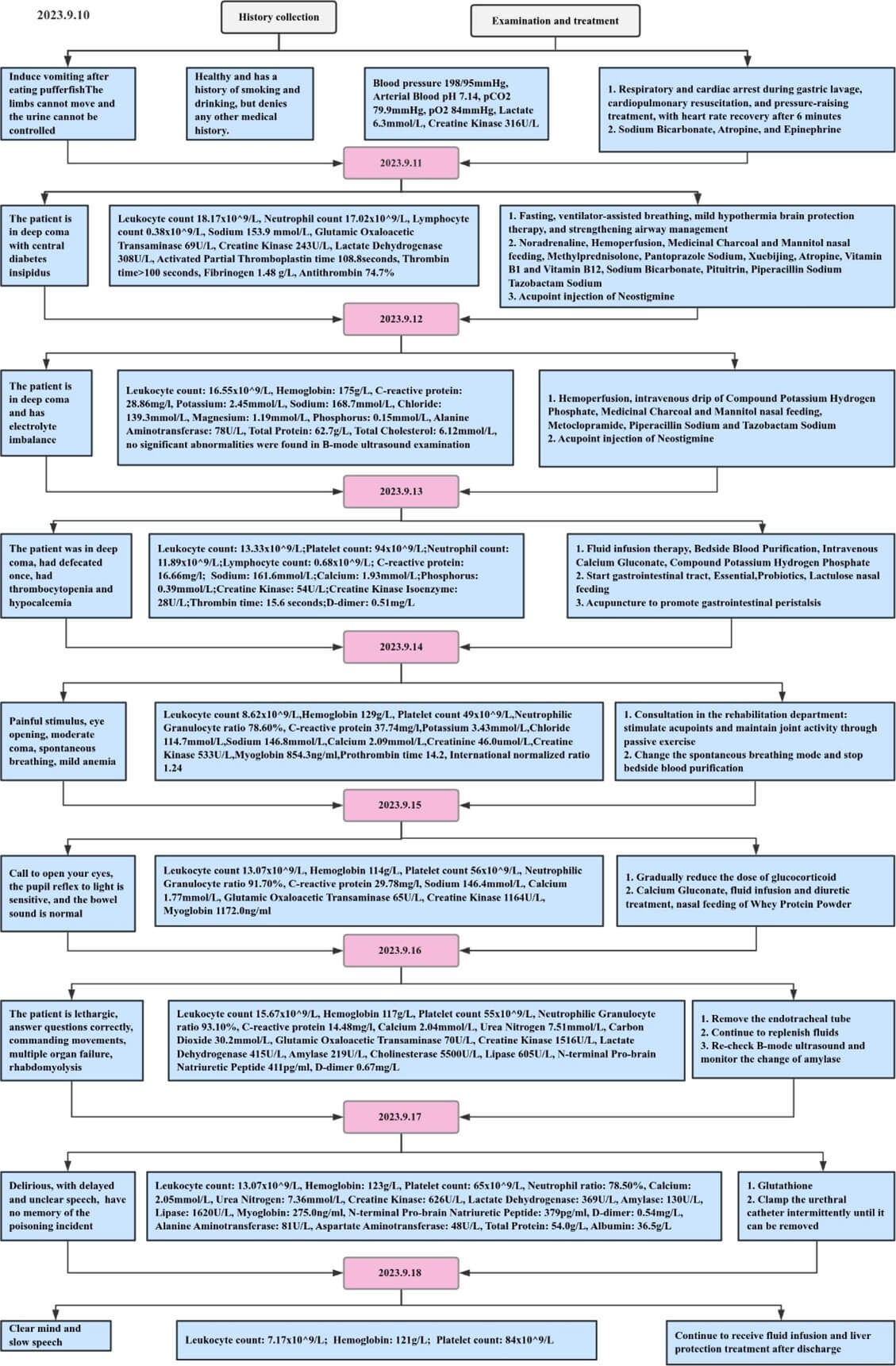
On September 11, 2023, the patient was in a deep coma. The respirator assisted breathing was performed, and Epinephrine was pumped into the bloodstream to increase pressure. Bedside blood was perfused, and 9 g of Medicinal Charcoal and 250 ml of Mannitol were absorbed by nasal feeding. 40 mg of Methylprednisolone was administered intravenously three times a day to purified and detoxified the blood. 40 mg of Pantoprazole Sodium was administered intravenously to alleviate the local irritation of the drug. Atropine was administered intravenously, 0.1 g of Vitamin B1 and 500 mg of Vitamin B12 were administered intramuscularly to nourish the nerves. After 6 hours, the patient's urine output was about 900-1200 ml per hour, with 18.17 × 109/L of white blood cells. Considering the patient's central diabetes insipidus and inhalation pulmonary infection, the patient was treated with Posterior Pituitary Hormone pump, Piperacillin Sodium Tazobactam Sodium 3.375 g once every 8 hours, and 1 ml of Neostigmine was injected into acupoint called Zusanli to prevent diuresis, inflammation, and promote excretion.
On September 12, 2023, the patient remained in a deep coma, with a 24-hour intake of 6164 ml, an outflow of 6109 ml, Potassium 2.45 mmol/L, Sodium 168.7 mmol/L, and Phosphorus 0.15 mmol/L. After enema, there was no defecation and other signs were stable. Maintained 0.30 ug/kg/min of Epinephrine, blood perfusion, Metoclopramide, and Piperacillin Sodium Tazobactam Sodium, Medicinal Charcoal and Mannitol nasal feeding adsorption, injection of Neostigmine into Zusanli, Composite Potassium Hydrogen Phosphate supply electrolyte.
On September 13, 2023, the patient had electrolyte disorders and Calcium was 1.93 mmol/L. Blood purification treatment, intravenous injection of calcium gluconate, and intravenous drip of Compound Potassium Hydrogen Phosphate were performed.
The patient defecated once, and the gastrointestinal tract was initiated. Gastrointestinal decompression was stopped, and 62.5 g of Health Factors, 2 g of Probiotics, and 15 ml of Lactulose were given nasogastric feeding. Acupuncture and Traditional Chinese Medicine enema was used to promote gastrointestinal peristalsis. Nutrition was supplemented, intestinal flora was adjusted, defecation was promoted.
On September 14, 2023, pressing the acupoints stimulated by the human body with hands to produce passive movement to promote the rehabilitation of limb joints and muscles. The patient can open his eyes after pain stimulation. The pupils were of equal size and diameter, all of which were 5 mm, the light reflex disappeared. Intestinal sounds were active, and involuntary movements were observed in the upper limbs. No response was observed in the lower limbs. Autonomous breathing was restored, and the mode of autonomous breathing was changed. High flow oxygen therapy (flow rate of 45 L/min, FIO2 30%) was continued. The blood sodium was normal, platelets were reduced, and bedside blood purification treatment was stopped. Fluid supplementation was continued, and nasal feeding was strengthened to supplement nutrition, airway management, and sputum drainage were strengthened.
On September 15, 2023, the patient can open their eyes after hearing the call. The pain stimulation in both upper limbs could retract, while the pain stimulation in both lower limbs had involuntary movements. The GCS score was E3VTM4. The doctor suggested reducing the dosage of Glucocorticoids gradually. Continuation of fluid supplementation and diuresis promoted the excretion of toxins.
On September 16, 2023, the patient was drowsy, could answer questions correctly, had directive movements. GCS score of E4VTM6. The tracheal intubation was removed and fluid replacement continued.
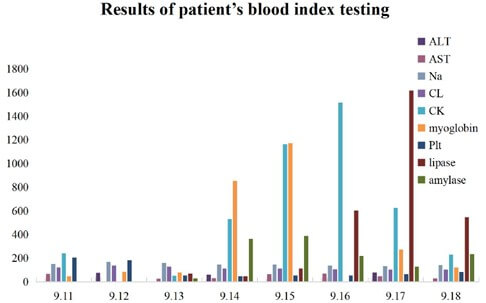
On September 17, 2023, the patient had sluggish speech, and liver function related enzyme detection were elevated. An additional dose of 1.6 g Glutathione was administered intravenously to protect the liver.
On September 18, 2023, the patient was clear and able to answer questions correctly. Remained sluggish speech, and his limb muscle strength was at level V with normal muscle tone. He was drowsy and had large and round pupils, and was sensitive to light reflection. The patient and his family insisted on being discharged from the hospital. The treatment process is shown in (Figure 2).
4. Examination of Tetrodotoxin Concentration
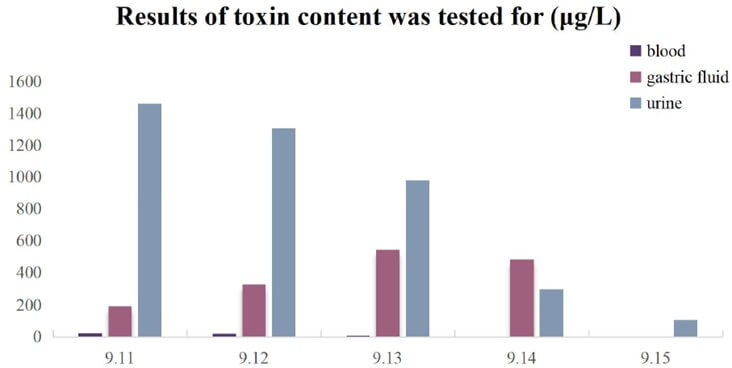
Samples of pufferfish, blood, gastric fluid, and urine were transferred to the Qinhuangdao Development Zone Center for Disease Control and Prevention for testing. After purification and separation, the samples were analyzed for tetrodotoxin concentration by Liquid Chromatography-Tandem Mass Spectrometer [6]. All samples contained high concentrations of tetrodotoxin. The average tetrodotoxin content of the remaining samples of pufferfish was found to be 47.36 mg/kg. The results of blood, gastric fluid and urine tests are shown in the (Figure 3).
5. Results
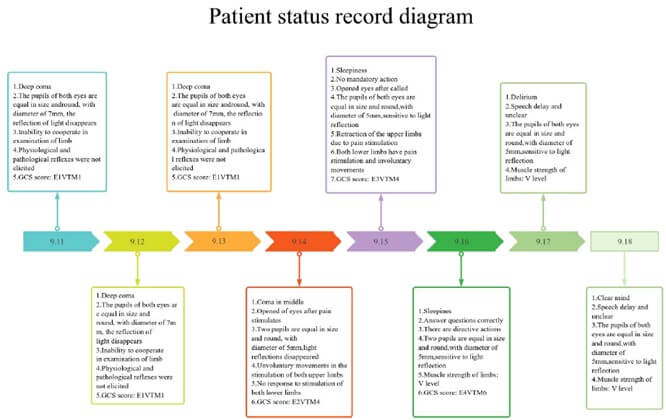
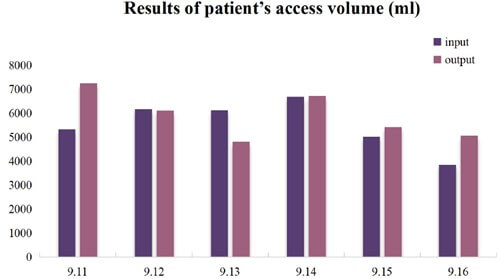
The patient was in deep coma when admitted to the hospital, with a GCS score of E1VTM1. Both pupils were equal in size and round, with a diameter of 7 mm. The patient showed no response to light reflex, and had normal muscle strength in the limbs. No physiological or pathological reflexes were elicited. The total intake was 5336 ml, and the total output was 7258 ml. The toxin levels in blood, gastric juice, and urine were 24.8, 191.6, and 1462 μg/L, respectively. At the time of discharge, the patient's expression was sluggish and his speech was not clear. Patient’ s pupils were equal in size and round, with a diameter of 5 mm, had sensitive light reflexes and a muscle strength of V in his limbs. The intake was 3856 ml and the output was 5055 ml. The toxin content in blood and urine was 1.2 and 108 μg/L, respectively. The results are shown in the (Figures 4-6).
In the end, after the unremitting efforts and meticulous treatment of the medical staff, the patient's vital signs, such as heart rate, blood pressure, respiratory rate and other key indicators, as well as nervous system responses, such as limb motor function, sensory function, nerve reflexes, etc., have gradually returned to normal levels after gradual adjustment and recovery, and the results of all reexaminations have been shown to be good, meeting the discharge criteria. The patient's awake state is shown in (Figure 7). The success of this treatment is mainly due to the fact that the hospital quickly activated the emergency response mechanism in the early stage of the patient's illness, opened up a green channel for the patient, so that he received a comprehensive and systematic examination and diagnosis in the shortest possible time, and immediately carried out targeted medical intervention. In the whole treatment process, the medical team conducted a meticulous analysis and evaluation of the patient's condition with rich clinical experience and professional knowledge, and adopted a scientific, reasonable and accurate treatment plan, from drug treatment to rehabilitation training, every link was rigorous, standardized and orderly, ensuring the accuracy and effectiveness of the treatment. It is precisely because of the combination of many factors such as the hospital's efficient treatment process, the superb medical skills of the medical team, and the all-round attentive care that the patient was able to recover in a relatively short period of time and finally be discharged from the hospital.

6. Discussion
6.1. Mechanism of the Pufferfish Poisoning
This article describes the treatment process after pufferfish poisoning. The patient initially experienced symptoms such as vomiting, numbness, cardiac arrest, and confusion. Part of the toxin is absorbed through the gastrointestinal tract, which stimulates the digestive system [7]. In addition, toxins that penetrate into the bloodstream act on the body, blocking the conduction process of Na ions, increasing the threshold of axons, reducing the amplitude of muscle action potentials and sensory nerve action potentials, and acting on the signal transmission of nerve systems and muscle systems, which can affect breathing, heartbeat, and limb movements [8].
The mortality rate of tetrodotoxin poisoning mainly depends on the amount of toxin ingested and whether treatment is timely. Currently, there is no clear detoxification plan for tetrodotoxin. Existing treatment options, such as respiratory support, have a very poor prognosis and there are no specific drugs. Even if they survive, the incidence rate of sequelae is high. In the recovery cycle, the intractable excitation conduction decreases, and the threshold of motor axon also has obvious abnormalities, which confirms that tetrodotoxin has difficult to recover effects on the human body by blocking nerve conduction, such as nervous system damage, respiratory system damage, digestive system damage, heart damage and liver damage [9].
6.2. Therapeutic and Outcomes of the Patient
The dosage in this case was more than three times the lethal concentration, but due to timely detection and treatment, a very significant therapeutic effect was achieved. If poisoning symptoms occur, seek medical treatment immediately to reduce the mortality and incidence rate of sequelae. In this case, the patient was treated with ventilator assistance for the respiratory system, and respiratory support plays a key role in the management of patients with tetrodotoxin poisoning [10]. Gavage, excretion promotion, blood perfusion, and fluid infusion are used to promote the metabolism of toxins outside the body. Studies have shown that the symptoms of poisoning improve significantly after hemodialysis. Renal dysfunction leads to accumulation of tetrodotoxin, which may affect the clinical course of tetrodotoxin poisoning [11]. During treatment, it is also necessary to focus on improving microcirculation, alkalizing blood, and using high-dose steroids to reduce the effect of toxins on tissues, prevent shock, brain edema, infectious stress ulcer, and other complications such as organ failure [12]. In addition, Traditional Chinese Medicine treatment with characteristics is conducive to the recovery of diseases, such as acupuncture and moxibustion, acupoint pressing auxiliary treatment to stimulate the recovery of nerve and muscle function, acupoint injection and Chinese Medicine to promote excretion.
7. Challenges
At present, people lack knowledge of the processing technology of pufferfish and the toxin content of pufferfish. China provides training and certification for the processing of pufferfish. However, after the death of pufferfish, the toxin will rapidly penetrate into the meat. There are significant differences in the concentration and tissue distribution of toxins among more than 100 species of pufferfish [13]. Professional personnel also have difficulty ensuring absolute safety, and it is necessary to raise people's awareness of potential safety hazards and take preventive measures.
Funding
Received funding from the Graduate Scientific Research and Innovation Project of Tianjin Education Commission (YJSKC-20201004).
Acknowledgements
This work has been supported by Qinhuangdao Development Zone Center for Disease Control and Prevention and Qinhuangdao Traditional Chinese Medicine Hospital.
Conflicts of Interest
None.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of Supporting Data
Data openly available in a public repository.
Author Contributions
Tong M.M: In-patient care, diagnostics and treatment. Wu M.X: Project administration, figure preparation, writing original draft, writing review & editing. Tao H.: In-patient care, diagnostics and treatment. Wang Y.H: Patient follow-up. Wu X.R: Detect the amount of tetrodotoxin. Tong M. M and Wang Y.H. contributed equally to this work.
Guarantor
Agree with the above.
REFERENCES
[1] Jie You, YaJun Yue, Feng Xing, et al. “Tetrodotoxin poisoning caused
by Goby fish consumption in southeast China: a retrospective case series
analysis.” Clinics (Sao Paulo),
vol. 70, no. 1, pp. 24-29, 2015. View at: Publisher Site | PubMed
[2] M Suehiro “Historical review on
chemical and medical studies of globefish toxin before World War II.” Yakushigaku Zasshi,
vol. 29, no. 3, pp. 428-434, 1994. View at: PubMed
[3] H Nakayama “Pharmacology of
tetrodotoxin and molecular structure of sodium channel as its target molecule.”
Yakushigaku Zasshi,
vol. 29, no. 3, pp. 441-445, 1994. View at: PubMed
[4] Dinghua Liu, Jianyu Zhang, Bojun Han,
et al. “An electrophysiological
study of acute tetrodotoxin poisoning.” Cell
Biochem Biophys, vol. 59, no. 1, pp. 13-18, 2011. View
at: Publisher Site | PubMed
[5] M Suleiman, J Muhammad, J Jelip, T
William, et al. “AN OUTBREAK OF
TETRODOTOXIN POISONING FROM CONSUMING HORSESHOE CRABS IN SABAH.” Southeast Asian J Trop Med Public Health,
vol. 48, no. 1, pp. 197-203, 2017. View at: PubMed
[6] Yijia Tang, Jianqiao Xu, Le Chen, et al. “Rapid in vivo determination of fluoroquinolones in cultured puffer fish
(Takifugu obscurus) muscle by solid-phase microextraction coupled with liquid
chromatography-tandem mass spectrometry.” Talanta,
vol. 175, pp. 550-556, 2017. View at: Publisher Site | PubMed
[7] Ryuji Kaji, Hiroyuki Nodera “Puffer
fish poisoning, Guillain-Barre syndrome and persistent sodium channels.” Ann Neurol, vol. 57, no. 3, pp.
309, 2005. View at: Publisher
Site | PubMed
[8] Matthew C Kiernan, Geoffrey K
Isbister, Cindy S-Y Lin, et al. “Acute
tetrodotoxin-induced neurotoxicity after ingestion of puffer fish.” Ann Neurol, vol. 57, no. 3, pp.
339-348, 2005. View at: Publisher
Site | PubMed
[9] Geoffrey K Isbister, Julie Son, Frank
Wang, et al. “Puffer fish
poisoning: a potentially life-threatening condition.” Med J Aust, vol. 177, no. 11-12, pp. 650-653, 2002.
View at: Publisher
Site | PubMed
[10] Deng-Fwu Hwang, Tamao Noguchi
“Tetrodotoxin poisoning.” Adv Food Nutr
Res, vol. 52, pp. 141-236, 2007. View at: Publisher Site | PubMed
[11] Ryuma Nakashima, Yasuki Nakata,
Masafumi Kameoka, et al. “Case
of tetrodotoxin intoxication in a uremic patient.” Chudoku Kenkyu, vol. 20, no. 2, pp. 141-145, 2007. View
at: PubMed
[12] F R Chowdhury, H A M Nazmul Ahasan, A
K M Mamunur Rashid, et al.
“Tetrodotoxin poisoning: a clinical analysis, role of neostigmine and
short-term outcome of 53 cases.” Singapore
Med J, vol. 48, no. 9, pp. 830-833, 2007. View at: PubMed
[13] Jon
B Cole, William G Heegaard, Jonathan R Deeds, et al. “Centers for Disease Control and Prevention
(CDC).Tetrodotoxin poisoning outbreak from imported dried puffer
fish--Minneapolis, Minnesota, 2014.” SMMWR
Morb Mortal Wkly Rep, vol. 63, no. 51, pp. 1222-1225, 2015.
View at: PubMed