Received: Mon 17, Feb 2025
Accepted: Wed 05, Mar 2025
Abstract
The coexistence of intracranial tumors and aneurysms is very rare but possible. Several reports and case series have reported the presence of tumors such as meningiomas and adenomas in associated aneurysms next the primary lesion. Intra-tumoral aneurysm is an even rarer finding, with a reported incidence as low as 0.3-0.7% in association with meningiomas. Craniopharyngiomas are benign tumors originating from remnants of Rathke's pouch with a high "invasive" capacity to surrounding neurovascular structures. We present a 61-year-old female patient with a history of suprasellar craniopharyngioma (SAMI 3, extension to the lower half of the third ventricle) transcranial resection 20 years ago. During follow-up, she reported headache worsening and subjective decline in residual right eye visual function. In this case, the aneurysm was located within the craniopharyngioma, projecting superiorly from the AcommA complex. Careful microvascular dissection and clipping of the aneurysm was performed prior to further tumor resection to prevent potential rupture and associated complications. This case report remarks on the importance of considering the possible association between certain types of tumors and aneurysm presence to implement a correct surgical strategy and to be aware of the possible complications related to this pathology.
Keywords
Intratumural aneurysm, Craniopharyngiomas, microvascular dissection, meningioma
1. Introduction
The coexistence of intracranial tumors and aneurysms is very rare but possible. Several reports and case series have reported the presence of tumors such as meningiomas and adenomas in associated aneurysms next the primary lesion [1-4]. Although it is not known to date whether there is a causal relationship between both pathologies, it is hypothesized that local and regional inflammatory tumoral process and hemodynamic changes affect the regional vasculature leading to the aneurysm formation [5].
Intra-tumoral aneurysm is an even rarer finding, with a reported incidence as low as 0.3-0.7% in association with meningiomas [3].
Anterior communicating artery (AcommA) aneurysms represent the 15-40% of intracranial aneurysm and are probably the intracranial aneurysms more prone to rupture, finding them in only <15% as unruptured [6-9].
Craniopharyngiomas are benign tumors originating from remnants of Rathke's pouch with a high "invasive" capacity to surrounding neurovascular structures. Although these tumors are predominant in the pediatric population, their management represents a challenge due to the technical surgical difficulty and the associated pre- and postoperative morbidity in these patients [10].
This case report describes a patient with a suprasellar recurrent craniopharyngiomas and the incidental finding of an intra-tumoral AcommA aneurysm.
2. Case Presentation
We present a 61-year-old female patient with a history of suprasellar craniopharyngioma (SAMI 3, extension to the lower half of the third ventricle) transcranial resection 20 years ago. During follow-up, she reported headache worsening and subjective decline in residual right eye visual function.
On examination, she was alert and oriented; of talmologic examination reported movement and light detection with right eye, preserving superior nasal quadrant during campimetry; left eye was reported with amaurosis. The rest of the neurological examination was unremarkable. The patient had hypopituitarism managed with hormone replacement therapy by neuroendocrinology department.
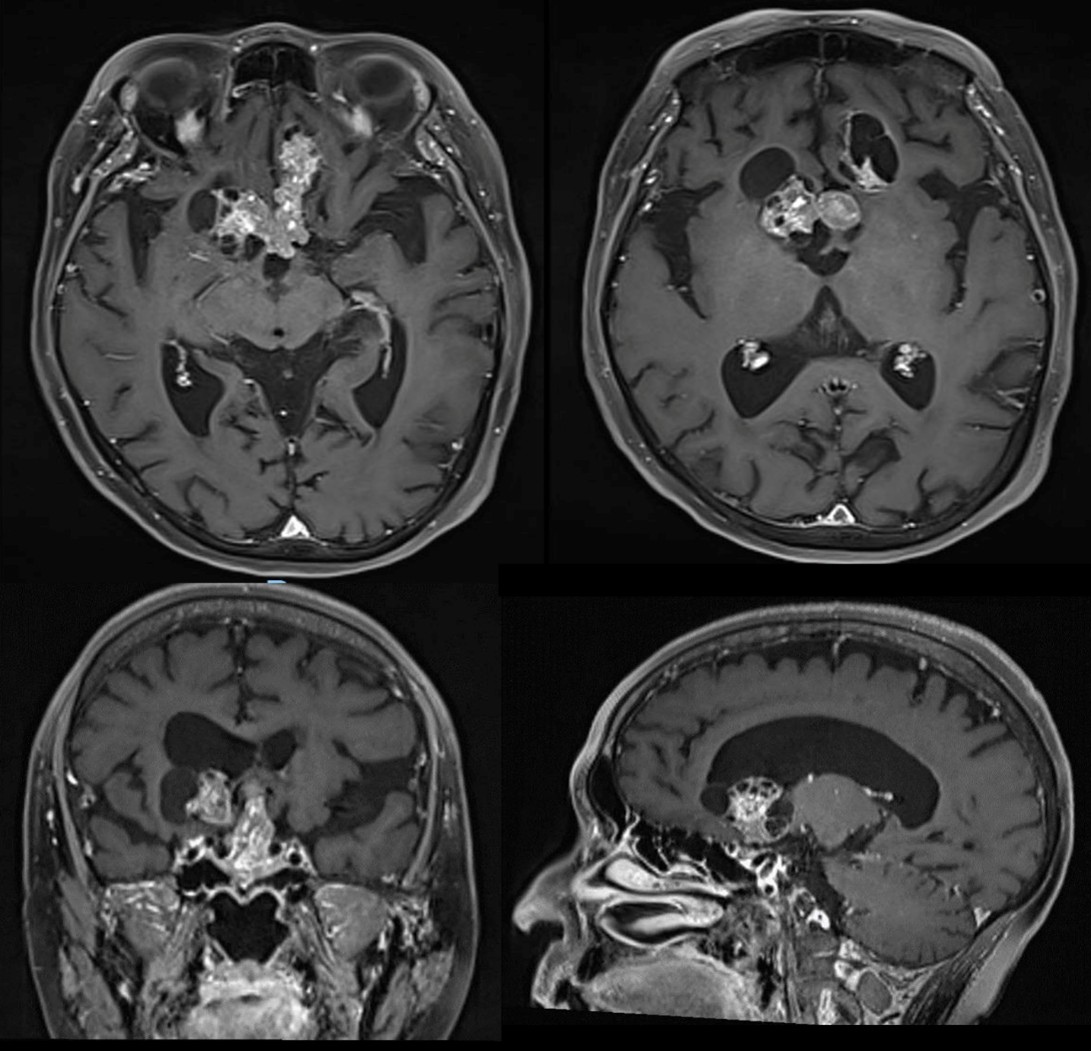
MRI with contrast confirmed tumor recurrence finding a predominantly suprasellar solid tumor significantly shifting upwards the third ventricle with anteriorly extension to the basal frontal gyrus in the anterior cranial fossa and a lateral cystic component (Figure 1). Surgical transcranial resection was decided.
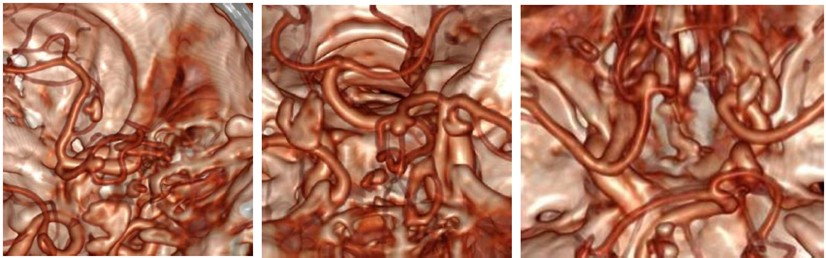
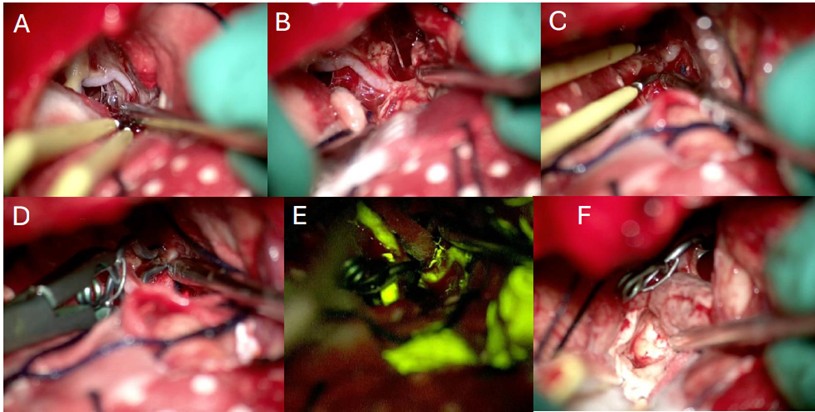
During surgery, the patient was placed in supine position with a neutral position of the head. A three-point fixation system and neuro-navigation system (BrainLab) were used. A bicoronal incision with bifrontal craniectomy were performed, using a subfrontal corridor for the tumor resection. Conventional microsurgery techniques were applied for initial tumor resection in its frontal extension; further dissection was carried out following anatomic landmarks until finding the arterial anterior communicating complex and the optic nerves surrounded by tumor. Careful dissection was then performed for the liberation of the optic apparatus continuing with the tumor resection between the quiasma and the AcommA (Figure 2). During this step a superior projection AcommA aneurysm was identified inside the solid central part of the tumor (video/imagen). After delimitation simultaneous tumor resection and dissection of the aneurysm was performed in order to clip it. After complete liberation of the aneurysm a 5 mm fenestrated clip was located in the neck of the lesion corroborating afterwards its complete occlusion using fluorescein. Haemostasis was confirmed, and closure was performed conventionally (Figure 3).
4. Discussion and Literature Review
This case report describes an adult patient with a recurrent craniopharyngioma in which an incidental AcommA aneurysm was found during surgical resection. The development of intra-tumoral aneurysms has been reported in various neoplasms, including meningiomas, pituitary adenomas, and craniopharyngiomas [11]. However, their occurrence in craniopharyngiomas is relatively rare, with an incidence estimated between 0.3-0.7%, likely due to the tumor's necrotic and cystic characteristics [12].
The precise mechanism linking tumor growth to aneurysm formation remains unclear, but several hypotheses have been proposed. Inflammation and oxidative stress produced by tumor secretion of cytokines like IL-6 may weaken vessel walls and contribute to aneurysm development [13]. Additionally, the mass effect of the tumor and its vascular supply may induce hemodynamic changes leading to aneurysm formation.
Qian et al. reported a case of a 41-year-old male with a craniopharyngioma, in whom an incidental blister-like aneurysm was found in the anterior communicating artery. In that case, an "8" type suture technique was performed, achieving total obliteration. The authors highlighted the possibility of a synergistic effect between the tumor and aneurysm formation, where cystic fluid may have leaked into the subarachnoid space, precipitating an inflammatory process and resulting in vascular wall remodelling and weakening [5].
In this case, the aneurysm was identified and clipped without incident, allowing for successful gross total resection of the recurrent craniopharyngioma. The presence of an intra-tumoral aneurysm poses additional challenges during surgery, requiring careful dissection and manipulation to avoid intraoperative rupture [14]. Preoperative imaging and meticulous surgical planning are crucial to identify and address vascular anomalies in patients with sellar and suprasellar lesions.
In this case, the aneurysm was located within the craniopharyngioma, projecting superiorly from the AcommA complex. Careful microvascular dissection and clipping of the aneurysm was performed prior to further tumor resection to prevent potential rupture and associated complications. While intra-tumoral aneurysms are rare in craniopharyngiomas, their recognition is crucial, as they may carry significant risk of rupture and hemorrhage during surgical manipulation. Meticulous microvascular techniques, including temporary clipping, may be necessary to safely resect the tumor and associated vascular pathology.
5. Conclusion
This case report remarks on the importance of considering the possible association between certain types of tumors and aneurysm presence to implement a correct surgical strategy and to be aware of the possible complications related to this pathology. Nowadays there is a lack of information about the pathophysiological association of these entities, therefore, future studies and reports are necessary to objectively establish this relation and to generate a deeper understanding of the vascular changes associated with the “tumor environment”.
Conflicts of Interest
None.
REFERENCES
[1] J
Handa, I Matsuda, H Handa “Association of brain tumor and intracranial
aneurysms.” Surg Neurol, vol. 6, no. 1, pp. 25-29, 1976. View at: PubMed
[2] H
W Pia, S Obrador, J G Martin “Association of brain tumours and arterial
intracranial aneurysms.” Acta Neurochir (Wien), vol. 27, no. 3, pp.
189-204, 1972. View at: Publisher
Site | PubMed
[3] Vijayakumar
Javalkar, Bharat Guthikonda, Prasad Vannemreddy, et al. “Association of
meningioma and intracranial aneurysm: report of five cases and review of
literature.” Neurol India, vol. 57, no. 6, pp. 772-776, 2009. View at: Publisher Site | PubMed
[4] Costanzo
De Bonis, Roberto Gazzeri, Leonardo Gorgoglione, et al. “Aneurysm inside
meningioma: an unusual association.” Br J Neurosurg, vol. 37, no. 3, pp.
294-295, 2023. View at: Publisher Site | PubMed
[5] Hai
Qian, M. P. (2019). Intraoperative Finding of an Anterior Communicating Artery
Blister-Like Aneurysm During a Primary Craniopharyngioma Resection: Accidental
or Incidental? World Neurosurg, vol. 127, pp. 514-517, 2019. View
at: Publisher Site | PubMed
[6] Hai-Tao
Lu 1, Hua-Qiao Tan, Bin-Xian Gu, et al. “Risk factors for multiple intracranial
aneurysms rupture: a retrospective study.” Clin Neurol Neurosurg, vol.
115, no. 6, pp. 690-694, 2013. View at: Publisher Site | PubMed
[7] Makio
Kaminogo, Masahiro Yonekura, Shobu Shibata “Incidence and outcome of multiple
intracranial aneurysms in a defined population.” Stroke, vol. 34, no. 1,
pp. 16-21, 2003. View at: Publisher Site | PubMed
[8] Ali
F Krisht, Jorge Gomez, Sharon Partington “Outcome of surgical clipping of
unruptured aneurysms as it compares with a 10-year nonclipping survival
period.” Neurosurgery, vol. 58, no. 2, pp. 207-216, 2006. View at: Publisher Site | PubMed
[9] Junhui
Chen, Mingchang Li, Xun Zhu, et al. “Anterior Communicating Artery Aneurysms:
Anatomical Considerations and Microsurgical Strategies.” Front Neurol,
vol. 11, pp. 1020, 2020. View at: Publisher Site | PubMed
[10]
Eva Venegas, Blanco Concepcion, Tomas
Martin, et al. “Practice guideline for diagnosis and treatment of
craniopharyngioma and parasellar tumors of the pituitary gland.” Endocrinol
Nutr, vol. 62, no. 1, pp. e1-e13, 2015. View at: Publisher Site | PubMed
[11]
Joao Paulo Almeida, Aristotelis
Kalyvas, Nilesh Mohan, et al. “Current Results of Surgical Treatment of
Craniopharyngiomas: The Impact of Endoscopic Endonasal Approaches.” World
Neurosurg, vol. 142, pp. 582-592, 2020. View at: Publisher Site | PubMed
[12]
Nelson Moussazadeh, Vishaal Prabhu,
Evan D Bander, et al. “Endoscopic endonasal versus open transcranial resection
of craniopharyngiomas: a case-matched single-institution analysis.” Neurosurgical
Focus, vol. 41, no. 6, pp. E7, 2016. View at: Publisher Site | PubMed
[13]
Onur Ozgural, Gokmen Kahilogullari,
Ihsan Dogan, et al. “Single-Center Surgical Experience of the Treatment of
Craniopharyngiomas With Emphasis on the Operative Approach: Endoscopic
Endonasal and Open Microscopic Transcranial Approaches.” J Craniofac Surg,
vol. 29, no. 6, pp. e572-e578, 2018. View at: Publisher Site | PubMed
[14] Bin Tang, Limin Xiao, Shenhao Xie, et al. “Extended endoscopic endonasal approach for recurrent or residual symptomatic craniopharyngiomas.” Clin Neurol Neurosurg, vol. 168, pp. 38-45, 2018. View at: Publisher Site | PubMed